
Translate this page into:
Anemic retinopathy in a patient with abdominal tuberculosis: A case report

*Corresponding author: Iku Dutt, Department of Ophthalmology, Regional Institute of Ophthalmology, GMCH, Guwahati, Assam, India. ikudutt@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Dutt I, Karak RK, Devi P. Anemic retinopathy in a patient with abdominal tuberculosis: A case report. J Ophthalmic Res Pract. 2024;2:19-23. doi: 10.25259/JORP_42_2023
Abstract
Retinal hypoxia caused by anemia can be a cause of retinal nerve fiber infarction and increased transmural pressure. This results in superficial and deep hemorrhages, cotton wool spots, retinal edema, Roth spots, and vessel dilatations. Tuberculosis (TB) may cause anemia due to malabsorption, reduced intake, or due to chronic diseased state. Here, we report a patient of abdominal TB with anemic retinopathy, which was improved after taking proper treatment for anemia.
Keywords
Anemic retinopathy
Abdominal tuberculosis
Roth spots

INTRODUCTION
A reduction in red blood cell (RBC) count, hemoglobin, and reduced hematocrit causes anemia. This results in reduced oxygen carrying capacity of blood which affects the body tissue. Retinal hypoxia caused by anemia can be a cause of retinal nerve fiber infarction and increased transmural pressure. This results in superficial and deep hemorrhages, cotton wool spots, retinal edema, Roth spots, and vessel dilatations. Anemic retinopathy may often be asymptomatic or may present with various retinal findings such as retinal hemorrhage, tortuous vessels, cotton wool spots, and sometimes pale-centered hemorrhages known as Roth spots. Carraro et al. reported that when hemoglobin is <8 g/dL, the incidence of Roth spot was found to be 28%. When hemoglobin is <6 g/dL, there is a steep rise in the incidence of retinopathy. Accompanying thrombocytopenia increases the incidence to 38%.[1] Along with systemic features of anemia per se (dizziness, fatigue, and malaise), ocular findings may be grouped according to the cause of anemia.[2] Tuberculosis (TB) is an infection caused by Mycobacterium tuberculosis. It is particularly common in developing countries like India where people live in crowded homes, unhealthy living conditions, and have insufficient access to health-care services.[3] TB can affect any organ system of our body and the abdomen is the sixth most common site. The site of involvement of abdominal TB can be intestine, lymph nodes, or peritoneum.[4] Studies have reported anemia in 61.53% of subjects with TB. The overall prevalence of severe, moderate, and mild anemia is 11.6%, 31.1%, and 35.67%, respectively.[5] Causes of anemia can be varied such as iron deficiency, chronic inflammation, and recurrent TB.[6] We report a case presenting with anemic retinopathy and abdominal TB in a 42-year-old man which improved after proper treatment for anemia.
CASE REPORT
A 42-year-old male reported to the medicine outpatient department of our hospital having chief complaints of generalized weakness, loss of appetite, and weight loss with intermittent fever for the past three months. The patient was referred to the Ophthalmology Department for dimness of vision in both eyes which was insidious in onset and gradually progressive for the past one month. General examination of the patient was unremarkable. His blood pressure was measured to be 130/80 mmHg, pulse rate was 105 beats/minute (min), respiratory rate of 22/min, and he had a temperature of 100°F. His visual acuity was finger counting at 5 m in both eyes not improving on pinhole. Anterior segment evaluation revealed pallor in both eyes and all other findings were normal [Figures 1 and 2].
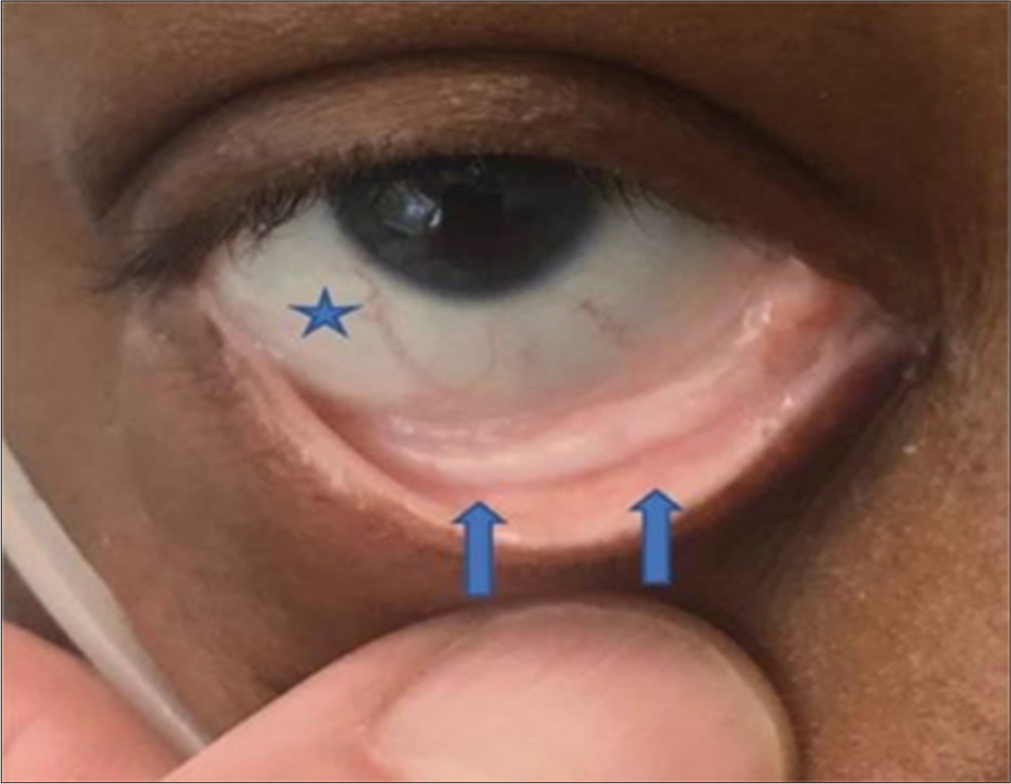
- Conjunctival pallor (arrows and star).
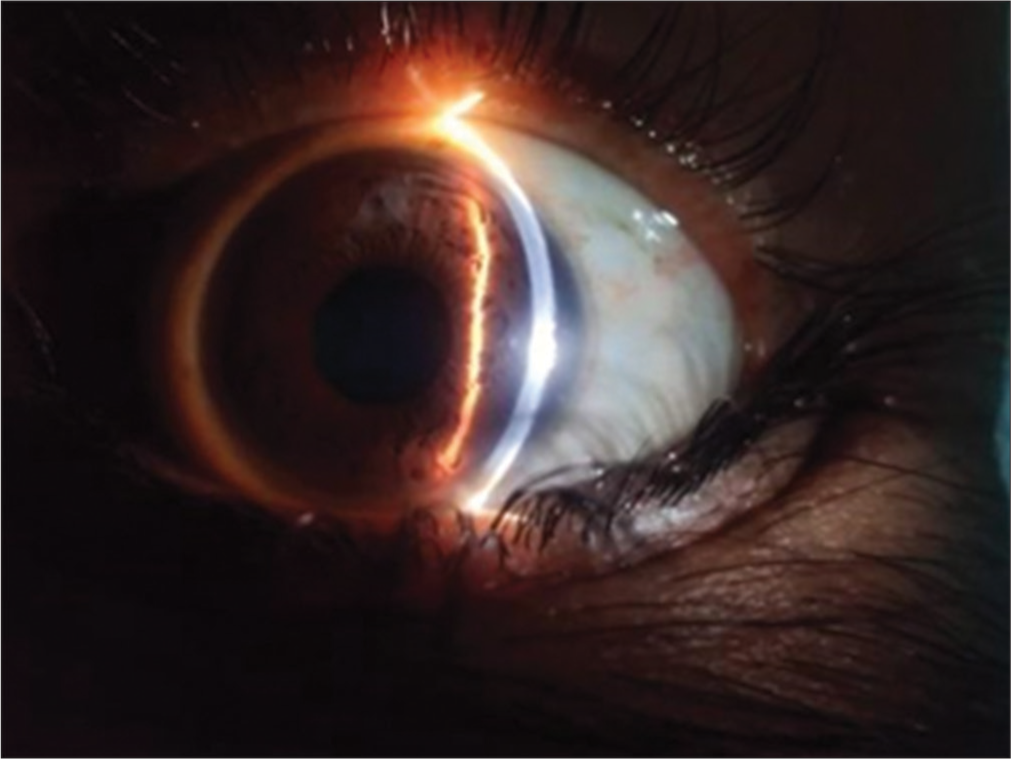
- Anterior segment.
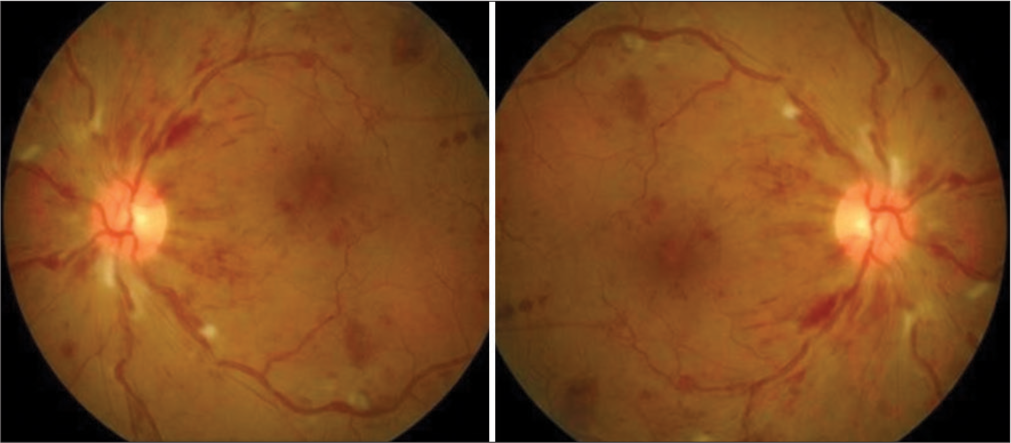
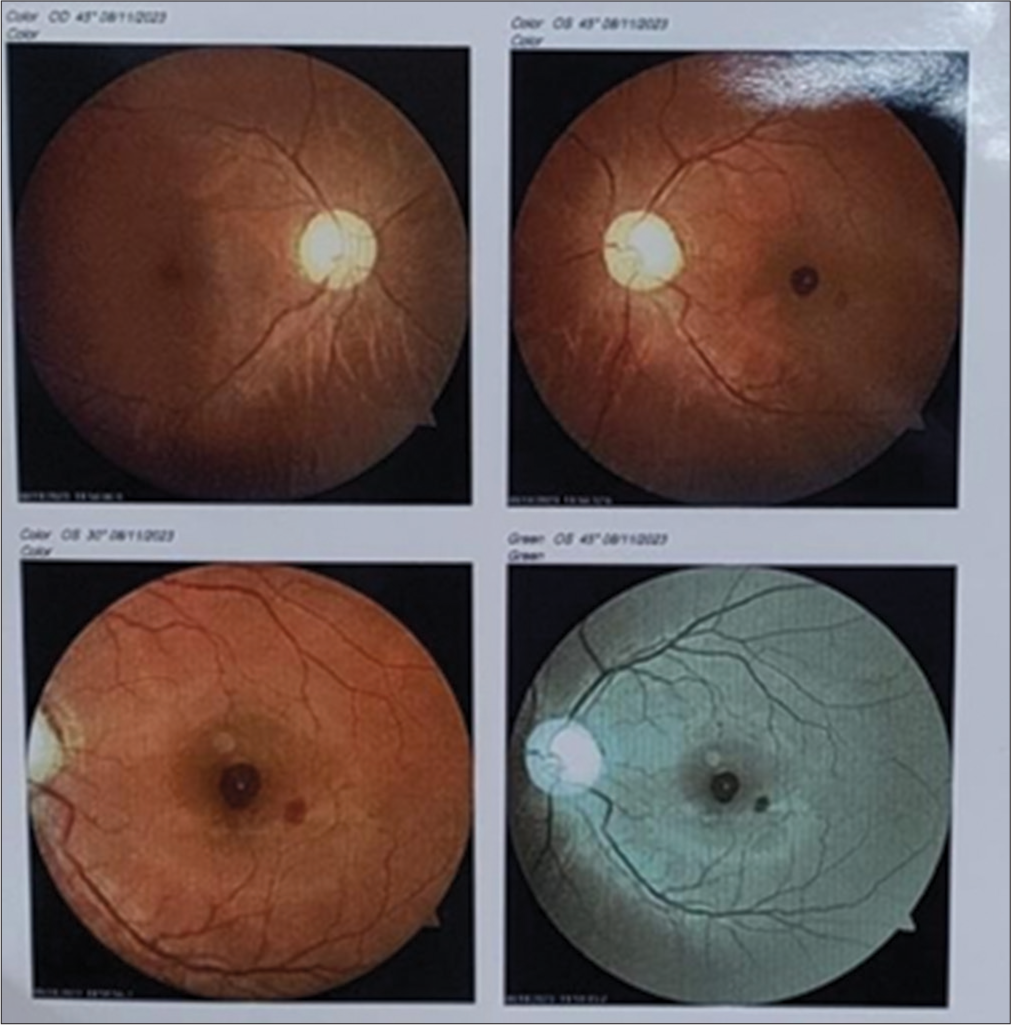
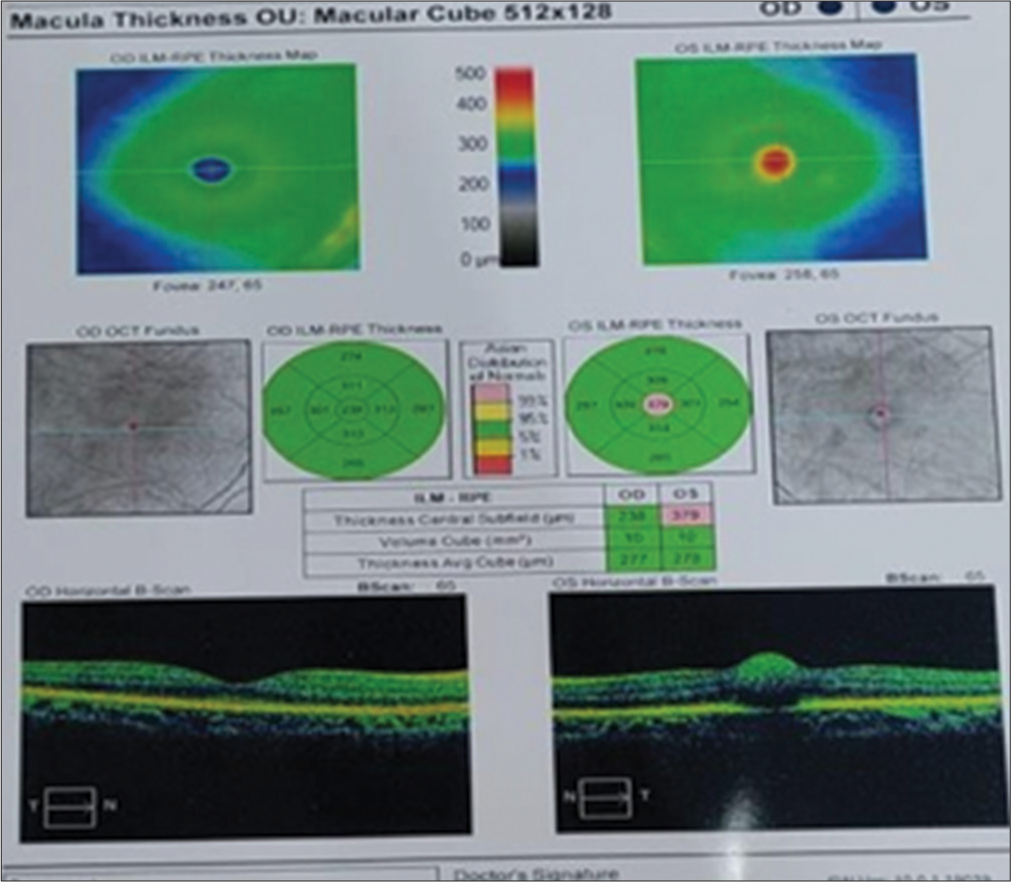
Intraocular pressure was 20 mmHg in both eyes. Fundus evaluation with 90 diopter retinal lens and indirect ophthalmoscopy showed Roth spots, superficial and deep hemorrhages, subhyaloid hemorrhage, and tortuous vessels. The optic disc showed a normal cup-to-disc ratio with a normal neuroretinal rim. Peripheral retinal examination was insignificant. Optical coherence tomography (OCT) of both eyes was done which revealed an increase in central foveal thickness with intraretinal and subretinal fluid collection. A vitreomacular traction was also seen [Figure 3].
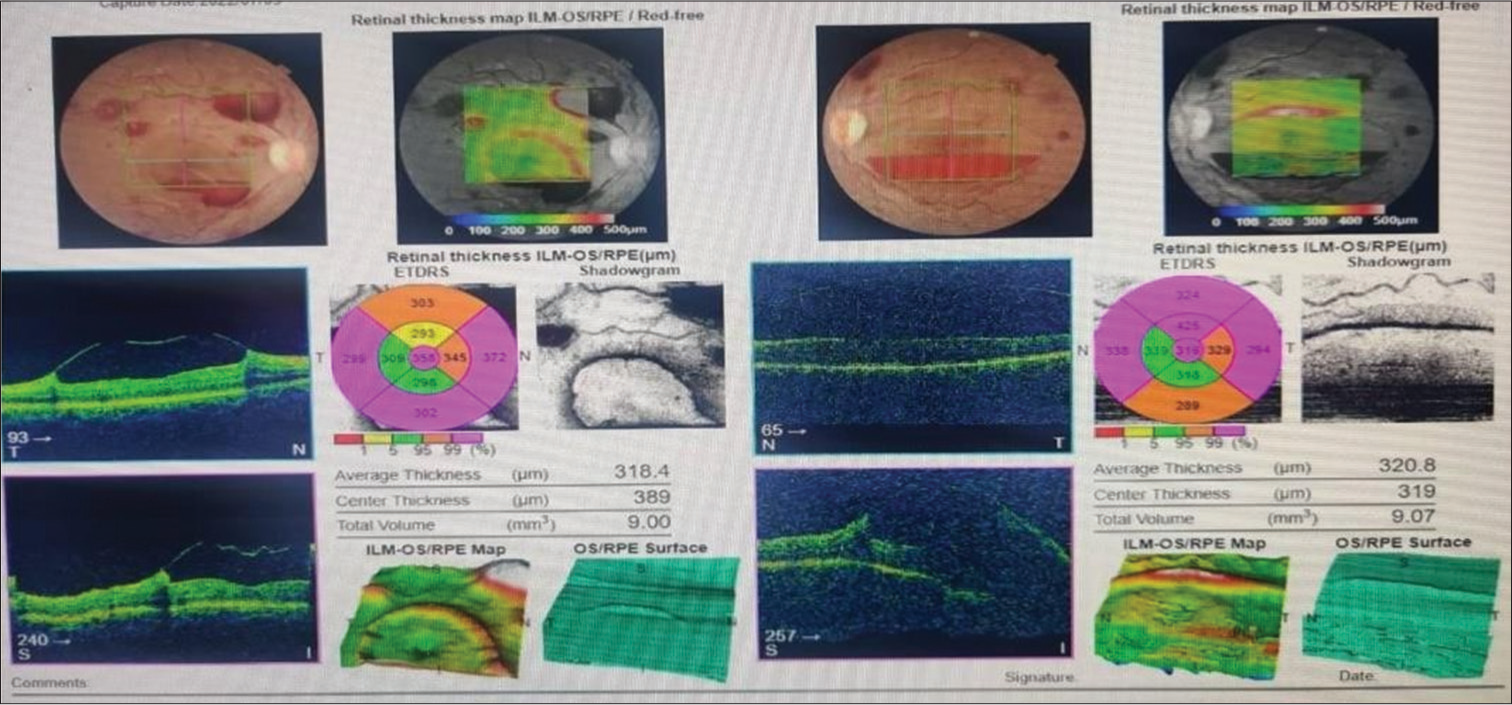
- Fundus photography and optical coherence tomography at the time of presentation.
Perimetry could not be done as the vision was very poor. His hemoglobin was 6.5 g/dL with peripheral blood smear showing normocytic normochromic cells with few macrocytes and mild anisocytosis. Erythrocyte sedimentation rate was 140 mm at the end of first hour, total white blood cell count was 2230/cu mm, platelet count was 2.43 lakhs/cu mm, Plasmodium falciparum/Plasmodium vivax (Malarial Parasite rapid test) was negative, and Salmonella Typhi immunoglobulin G and M (IgG and IgM) were non-reactive. His liver function test showed elevated aspartate aminotransferase (100U/L), random blood sugar (RBS) 170 mg/dL, serum urea 40.6 mg/dL, and serum creatinine 1.04 mg/dL. His blood for viral markers hepatitis B surface antigen, anti-hepatitis C virus, human immunodeficiency virus (HIV) 1, and HIV 2 antibodies were negative. Enzyme-linked immunoassay for anti-dengue antibody, IgG and IgM, was non-reactive. Both direct and indirect Coomb’s test was negative. His chest X-ray was normal.
Contrast-enhanced computed tomography abdomen revealed features suggestive of retroperitoneal abdominal and inguinal lymphadenopathy with mild splenomegaly. Inguinal lymph node biopsy shows features of caseating granuloma with giant cells and epithelial cells [Figures 4-7].
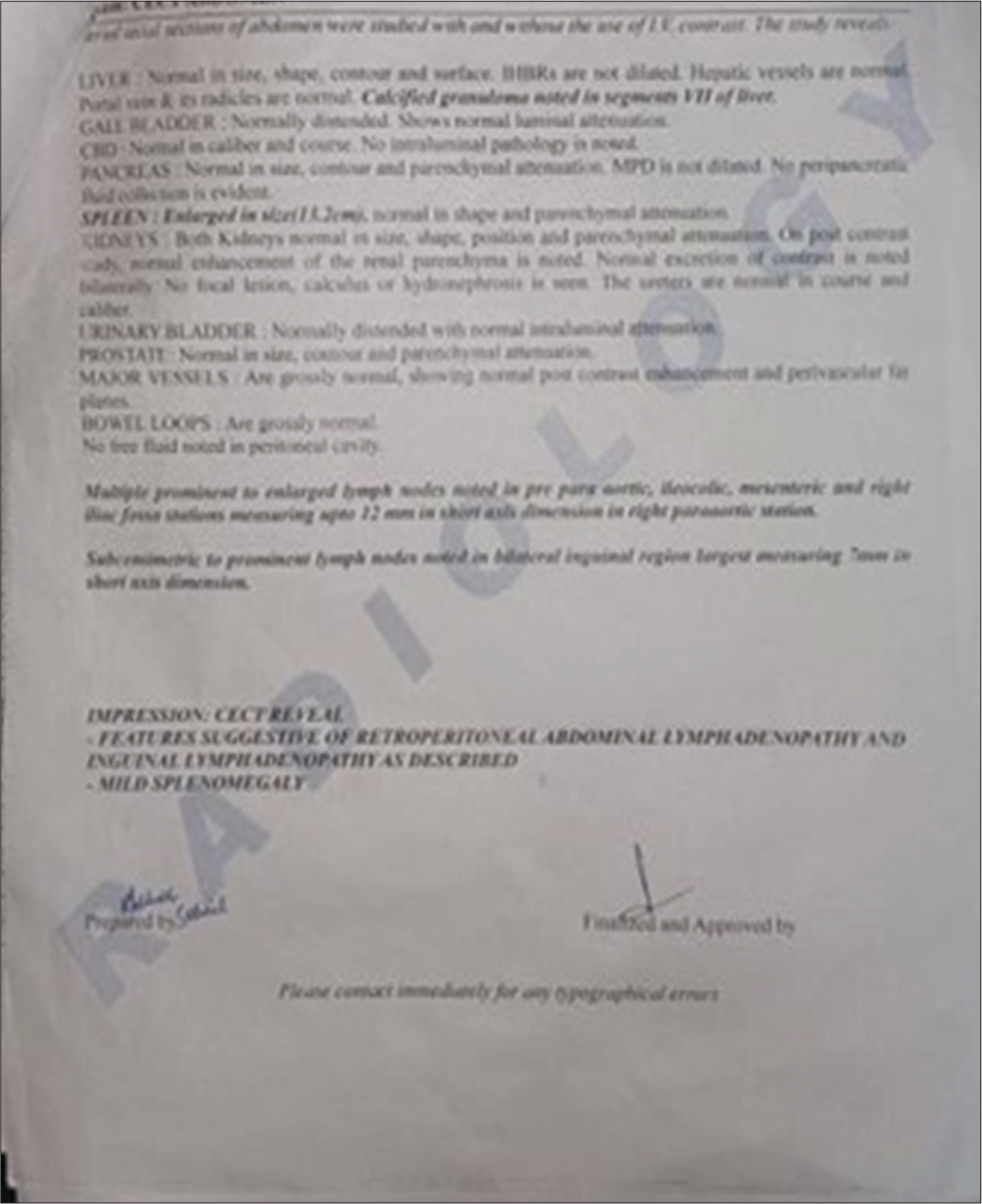
- Contrast-enhanced computed tomography abdomen report.
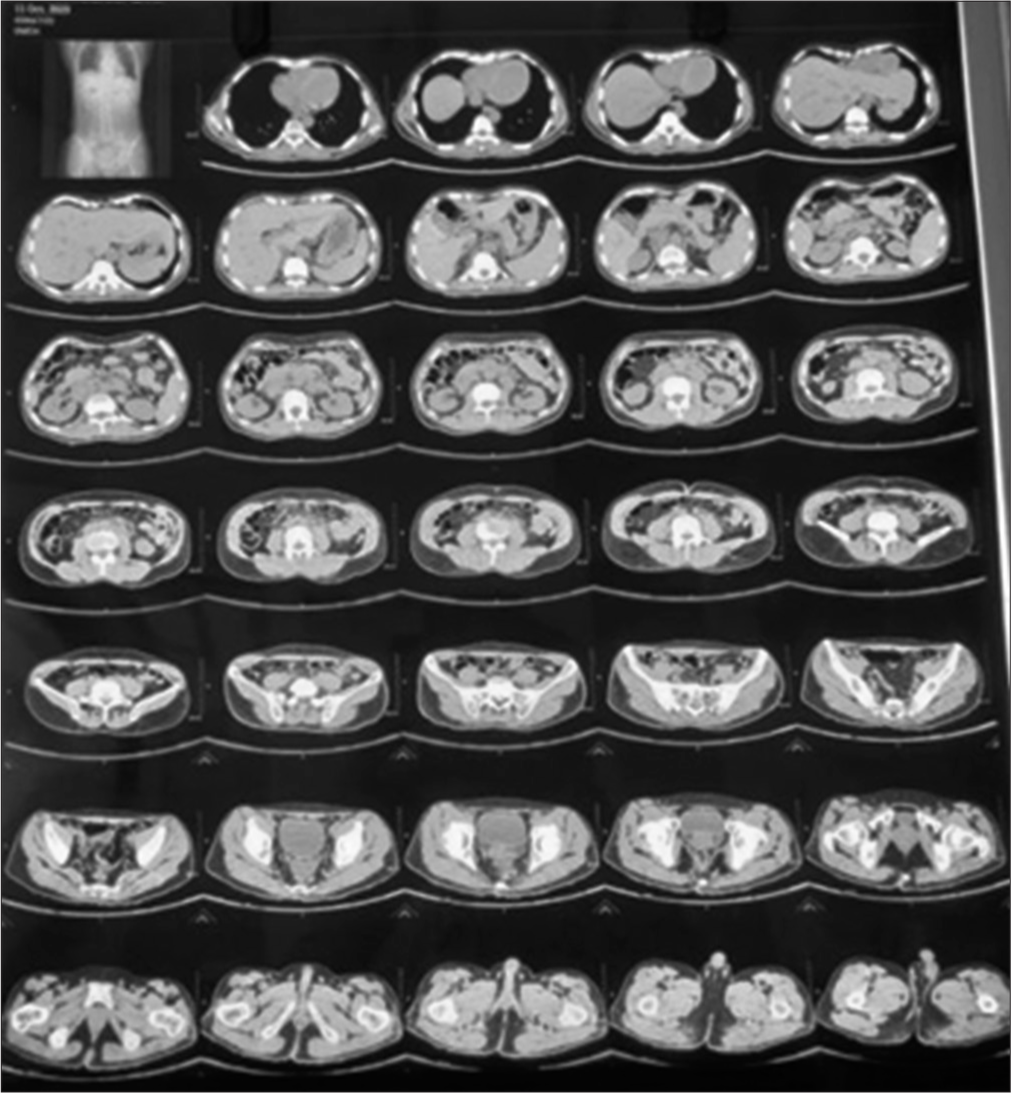
- Contrast-enhanced computed tomography abdomen flim.
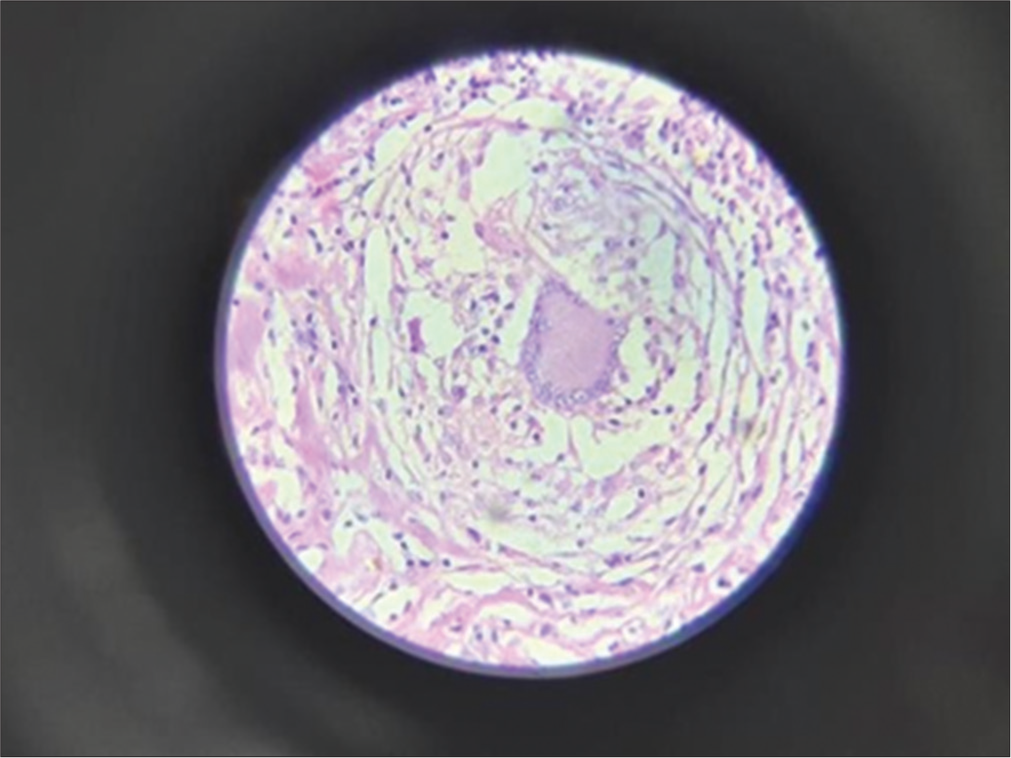
- Tuberculosis granuloma HPE.
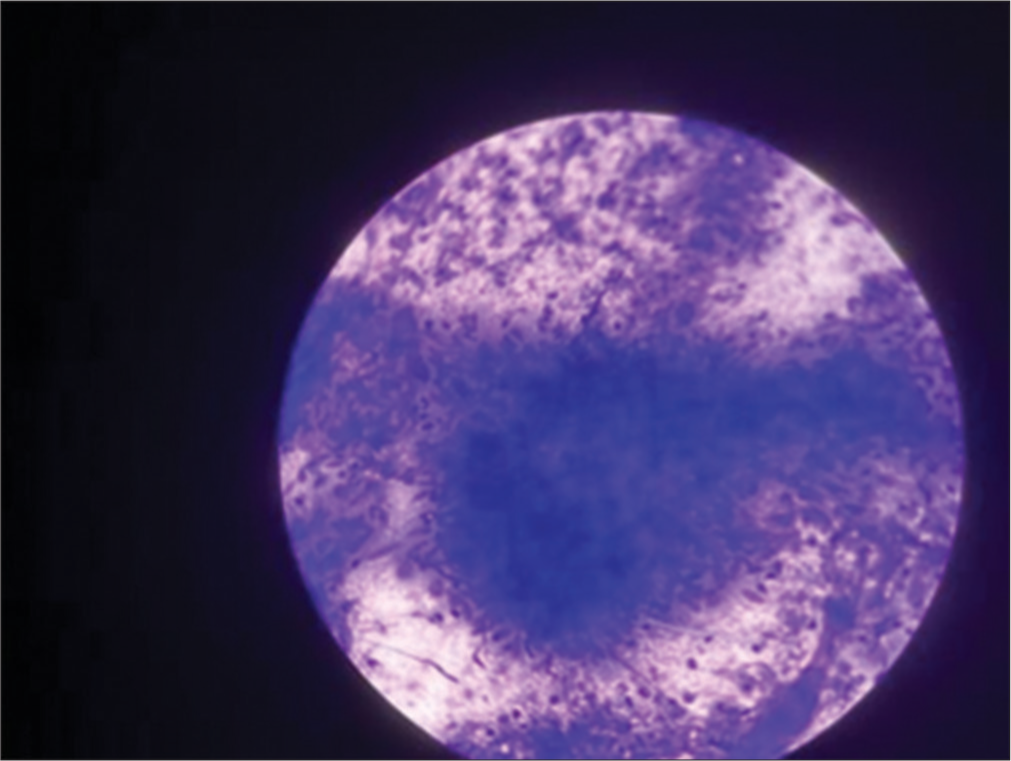
- Tuberculosis cytology report.
Cartridge-based nucleic acid amplification test (CBNAAT) for TB was found to be positive. The patient was started on anti-tubercular treatment with fortified iron folic acid tablets, injection ceftriaxone, and aminowel infusion by the medicine department. We started the patient on eye drop Nepafenac 1 drop 3 times a day both eyes and tablet Vitamin C and antioxidant 1 tablet once daily for 2 months. The patient received 3 units of packed RBC of blood group A+. After 4 weeks, the patient showed improvement in his vision with visual acuity 6/36 (P) and 6/60 in the right and left eye, respectively. There was a resolution of superficial hemorrhages and Roth spots. His hemoglobin was improved to 9.4 g/dL.
The patient was followed regularly for six months every month. After 10 weeks, the visual acuity improved to 6/9 (p) and 6/36 (p) in the right and left eye, respectively. The fundus picture shows the resolution of hemorrhages in the right eye and one macular hemorrhage in the left eye [Figures 8-10].
- Fundus picture of the patient after 4 weeks starting treatment.
- Fundus picture of the patient after 10 weeks of treatment.
- Optical coherence tomography after 10 weeks of treatment.
Right eye OCT was normal and the left eye showed increased foveal thickness with sub-retinal fluid.
DISCUSSION
Anemic retinopathy is often an incidental finding resulting from varied systemic conditions.[7]
Fundus picture shows hemorrhages, venous dilatation, and nerve fiber layer infarctions occurring as a result of hypoxia. Anemia in TB occurs consequent to nutritional deficiency, chronic diseases, and malabsorption.[8] Malabsorption syndrome occurs in intestinal TB which involves the ileocecal region.[9] Anemia can be diagnosed by blood investigation such as hemoglobin, mean corpuscular volume, mean corpuscular hemoglobin, hematocrit, mean corpuscular hemoglobin concentration, and abdominal TB with CBNAAT and lymph node biopsy. In our case, the patient had anemic retinopathy with abdominal TB, who after treatment showed resolution of retinopathy with visual improvement.
CONCLUSION
Both anemia and TB have a high prevalence in India, although both may present differently. It is essential for all health-care professionals to keep an eye on such situations. Retinopathy of anemia tends to be asymptomatic, so a thorough multipronged systemic approach is needed to ensure a favorable result and avoid co-morbidities.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consents.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Prevalence of retinopathy in patients with anaemia or thrombocytopenia. Eur J Haematol. 2001;67:238-44.
- [CrossRef] [PubMed] [Google Scholar]
- Abdominal tuberculosis in Bradford, UK: 1992-2002. Eur J Gastroenterol Hepatol. 2005;17:967-71.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of anaemia among patients with tuberculosis: A systemic review and meta-analysis. Indian J Tuberc. 2019;66:299-307.
- [CrossRef] [PubMed] [Google Scholar]
- Tuberculosis-associated anaemia is linked to a distinct inflammatory profile that persists after initiation of antitubercular therapy. Sci Rep. 2019;9:1381.
- [CrossRef] [PubMed] [Google Scholar]
- Severe anaemic retinopathy in primitive neuroectodermal tumour. BMJ Case Rep. 2019;12:e230365.
- [CrossRef] [PubMed] [Google Scholar]
- Immune haemolytic anaemia in a patient with tuberculous lymphadenitis. J Glob Infect Dis. 2011;3:89-91.
- [CrossRef] [PubMed] [Google Scholar]
- Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. Vol 1. Philadelphia, PA: W.B. Saunders; 2015.
- [Google Scholar]




