
Translate this page into:
Eyes and beyond: Understanding Horner’s syndrome

*Corresponding author: Vidhya Nagasubramanian, Department of Orbit and Oculoplasty, The Eye Foundation, Coimbatore, Tamil Nadu, India. vidhyajr@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nagasubramanian V, Manivel P. Eyes and beyond: Understanding Horner’s syndrome. J Ophthalmic Res Pract. doi: 10.25259/JORP_42_2024
A 32-year-old female presented with complaints of right eyelid drooping that had gradually developed over the past year. She sought correction for improved symmetry. On examination, she had moderate ptosis covering the visual axis with a well-defined lid crease, and her levator palpebrae superioris function was excellent. There was no drooping or lid lag on the downgaze. Ocular movements were full. She also gave a history of diurnal variation of ptosis with slight worsening of ptosis in the evening. The ice pack test and fatigue test were equivocal. Anti-acetylcholine receptor antibody assays and repetitive nerve stimulation tests were negative for myasthenia gravis.
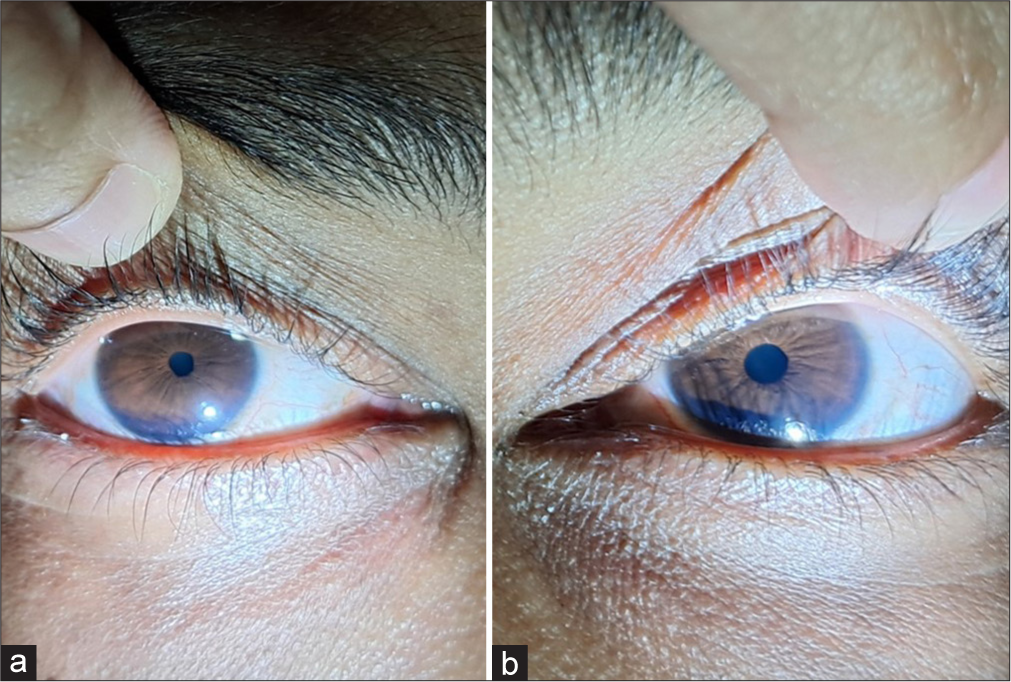
On further examination, the patient reported a history of upper limb deformity since birth and a recent onset of neck pain for which she had not sought treatment [Figure 1]. Her upper limb deformity was characteristic of Klumpke’s palsy, which can involve the brachial plexus. Anterior segment examination revealed right-sided anisocoria with a miotic pupil [Figures 2a and b]. Given the pupillary involvement, a topical phenylephrine test was performed with phenylephrine applied to the superior fornix. The ptosis was re-examined after 5 minutes, and the topical phenylephrine test showed complete resolution of the ptosis within that time [Figures 3a and b].

- Right-sided birth defect of upper limb and right-sided ptosis.
- (a and b) Right eye miotic pupil and left eye normal pupil.

- (a and b) Right-sided ptosis showing improvement after topical phenylephrine.
We made a clinical diagnosis of right-sided Horner’s syndrome and referred her for a comprehensive neurological evaluation. Imaging and neurological assessments confirmed cervical plexopathy due to a birth injury [Figure 4], with progressive cervical myelopathy. She was advised to undergo cervical discectomy.

- Cervical compression at the level of C5-C6.
Horner’s syndrome is a rare cause of ptosis resulting from lesions anywhere in the sympathetic pathway that supplies the head and neck.[1] The condition is primarily acquired, secondary to systemic or local diseases, or iatrogenic causes, but it can also be congenital and purely hereditary in rare cases. Typically, it presents as a triad of partial ptosis, miosis, and anhidrosis. Anhidrosis may be absent in incomplete Horner’s syndrome in lesions primarily involving the internal carotid artery.[1]
The syndrome was first described by Swiss ophthalmologist Johann Friedrich Horner in 1869 and has been referred to by various names, including Horner syndrome, Claude Bernard-Horner syndrome, oculosympathetic palsy, and von Passow syndrome (Horner syndrome in association with iris heterochromia).
The sympathetic pathway originates from the hypothalamus to the C8–T2 level in the spinal cord – referred to as first-order neurons. The second order, or preganglionic neurons, ascend from the T1 level of the spinal cord to enter the cervical sympathetic chain, which then terminates in the superior cervical ganglion at the C3-C4 level. The third order or postganglionic neurons ascend from the superior cervical ganglion and travel along the adventitia of the internal carotid artery into the cavernous sinus, and the oculosympathetic fibers exit the internal carotid artery in close proximity to the trigeminal ganglion and the sixth cranial nerve and join the 1st division of the trigeminal nerve to enter the orbit. The fibers (long ciliary nerve) innervate the dilator muscles of the iris, smooth muscle (Müller’s muscle), and the vasomotor and sudomotor fibers to the face. The etiology varies according to the site of the lesion as central and peripheral Horner’s syndrome.[2] In central Horner’s, the lesions are in first-order neurons, includes stroke, demyelination, and neoplasm. In peripheral Horner’s, the lesion can be preganglionic (second-order neurons) and post-ganglionic (third-order neurons). The preganglionic causes can be thoracic outlet syndrome, mediastinal tumors, Pancoast’s tumor, thyroid malignancies, and trauma involving the thoracic spinal cord or iatrogenic – due to surgical procedures in these regions. The postganglionic causes can be lesions of the superior cervical ganglion – trauma, radical neck dissection, internal carotid artery – dissection, thrombosis, and invasion by tumor.
The diagnosis of Horner’s syndrome is primarily clinical, with confirmation achieved through pharmacological tests following the application of topical drops such as cocaine, hydroxyamphetamine, and a 1:1000 dilution of adrenaline.[1] Topical phenylephrine, typically used to identify cases with a favorable prognosis for conjunctival Müller muscle resection, provides a valuable clinical clue indicating Müller muscle involvement, especially in the presence of a miotic pupil and characteristic hand deformity.
A few cases of acute Horner’s syndrome following cervical disc herniation have been reported.[3-5] Progressive cervical myelopathy likely led to the development of Horner’s syndrome in this patient, who already had a birth palsy characterized by hand deformity.
A critical aspect of the diagnosis is conducting a thorough systemic examination to identify any neurological signs, as some causes of Horner’s syndrome can present as urgent medical or surgical emergencies. A careful clinical examination, supplemented by appropriate pharmacological and radiological evaluations, solidifies the diagnosis and enhances patient management.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that they have used artificial intelligence (AI)-assisted technology to assist in the writing or editing of the manuscript or image creations.
Financial support and sponsorship: Nil.
References
- Horner syndrome: Clinical perspectives. Eye Brain. 2015;7:35-46.
- [CrossRef] [PubMed] [Google Scholar]
- Horner syndrome revisited: With an update of the central pathway. Clin Anat. 1999;12:345-61.
- [CrossRef] [Google Scholar]
- Cervical myelopathy presenting with an acute Horner's syndrome. Interdisciplin Neurosurg. 2019;17:19-22.
- [CrossRef] [Google Scholar]
- Horner syndrome associated with a herniated cervical disc: A case report. Korean J Spine. 2012;9:108-10.
- [CrossRef] [PubMed] [Google Scholar]
- Horner syndrome as an unusual presentation of cervical radiculomyelopathy associated with cervical disc herniation: A case report. Int J Surg Case Rep. 2023;110:108666.
- [CrossRef] [PubMed] [Google Scholar]




