
Translate this page into:
Eyes are the window to the brain!!


*Corresponding author: Anupama Janardhanan, Department of Paediatric Ophthalmology and Strabismus, Aravind Eye Hospital, Tirunelveli, Tamil Nadu, India. dranupamaj@outlook.com
-
Received: ,
Accepted: ,
How to cite this article: Janardhanan A, Rengappa V, Valentine R. Eyes are the window to the brain!! J Ophthalmic Res Pract. doi: 10.25259/JORP_32_2024
A 41-year-old female patient presented with the inability to move her eyes up for a day. She was a known case of ischemic heart disease on oral anticoagulants. On evaluation, her visual acuity in oculus dexter (OD), right eye was LogMar 0.18 and oculus sinister (OS), left eye was LogMar 0. She had mid-dilated, sluggish pupils in both eyes. There was a gross −4 limitation of elevation and −3 limitation of depression in both eyes. A convergence nystagmus was noted on attempted elevation. Her fundus evaluation was normal. She appeared mildly disoriented and dysarthric at the time of presentation. The patient underwent a detailed neurological assessment that revealed gait abnormalities. The patient showed Vertical gaze paresis of acute onset with pupillary involvement associated with ataxia. Hence, immediately within 1 day of the onset of symptoms, a magnetic resonance image and magnetic resonance angiography brain with contrast were advised. The patient was provisionally diagnosed with a possible cerebrovascular accident (CVA) and immediately referred for emergency care to the nearest multispecialty hospital. The patient was reviewed after 2 weeks with neuroimaging after systemic conservative management for CVA. Neuroimaging confirmed the provisional diagnosis made at the peripheral eye center. It showed an acute left-sided thalamo-capsular infarct, explaining the ocular and systemic features in the patient. On follow-up at 2 months, the patient showed improvement in gaze abnormalities and pupillary reaction [Figure 1a-g].
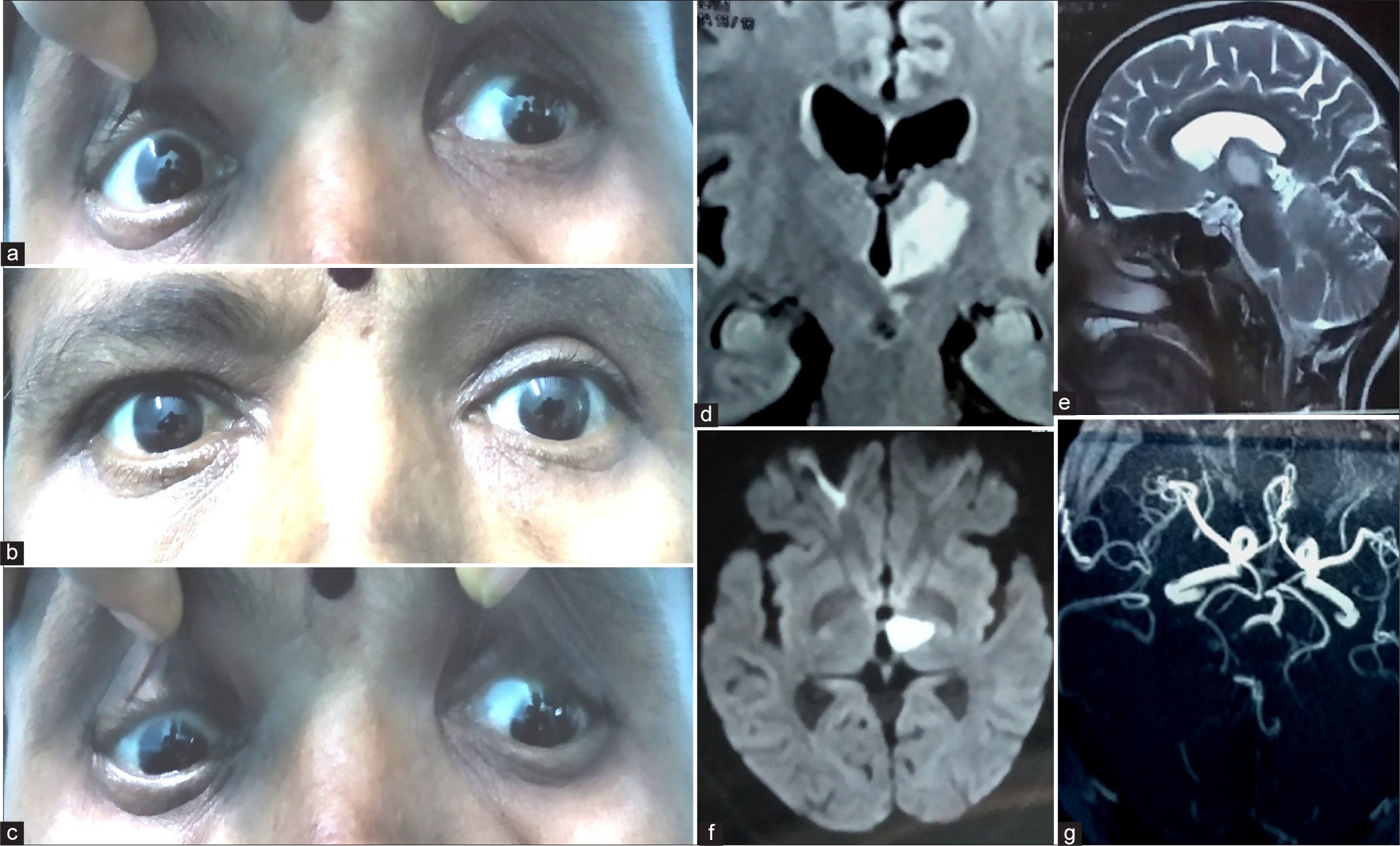
- (a-c) Upgaze, primary gaze, and downgaze images of the patient. (d) Coronal T2-weighted fluid-attenuated inversion recovery magnetic resonance (MR) image of the brain showing hyperintense area in the left thalamus. (e) Hyperintensity demonstrated in the left thalamus on sagittal T2-weighted image. (f) Axial diffusion-weighted Image showing high signal in the left thalamus. (g) MR angiogram of the patient.
The final diagnosis was vertical gaze paresis with pupil involvement secondary to thalamic infarct. Vertical gaze palsies have usually been attributed to midbrain lesions involving interstitial nucleus of Cajal and the rostral interstitial nucleus of the medial longitudinal fasciculus.[1] In our case, there was no midbrain involvement. This phenomenon is attributed loss of supranuclear control in such cases.[2] Patients with systemic comorbidities require strong suspicion of CVA and prompt multispecialty management to prevent mortality. Hemorrhagic transformation of ischemic strokes is commonly seen in patients on systemic anticoagulants.[3] As per Choi et al., thalamic strokes, evidenced radiologically, also show involvement of the dorsal midbrain pathologically confirmed on autopsies.[4] Pupillary involvement has been reported in thalamic hemorrhages; it has been theorized to be due to damage of the mesencephalic-diencephalic junction, possibly involving the convergence pathway and neurons.[5]
Ethical approval:
The Institutional Review Board approval is not required.
Declaration of patient consent:
The authors certify that they have obtained all appropriate patient consent.
Conflict of interest:
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation:
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- “Conjugate Gaze Palsies - Neurologic Disorders In: Merck Manuals Professional Edition. United States: Merck Sharp and Dohme Corp; 2015. Reviewed/Revised Nov 2023. Available from: https://www.msdmanuals.com/professional/neurologic-disorders/neuroophthalmologic-and-cranial-nerve-disorders/conjugate-gaze-palsies
- [Google Scholar]
- Vertical gaze palsies from medial thalamic infarctions without midbrain involvement. Stroke. 1995;26:1467-70.
- [CrossRef] [PubMed] [Google Scholar]
- Predictors of hemorrhagic transformation after acute ischemic stroke based on the experts' opinion. Arq Neuropsiquiatr. 2020;78:390-6.
- [CrossRef] [PubMed] [Google Scholar]
- Specificity of “peering at the tip of the nose” for a diagnosis of thalamic hemorrhage. Arch Neurol. 2004;61:417-22.
- [CrossRef] [PubMed] [Google Scholar]
- "Peering at the tip of the nose" as a sign of thalamic haemorrhage. Neuro Ophthalmol. 2014;38:21-3.
- [CrossRef] [PubMed] [Google Scholar]




