
Translate this page into:
Oculofacial esthetics in ophthalmology

*Corresponding author: Ashok Kumar Grover, Department of Oculoplastic Surgery, Vision Eye Centre, New Delhi, India. akgrover55@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Grover AK, Thomas R, Singh G. Oculofacial esthetics in ophthalmology. J Ophthalmic Res Pract 2023;1:52-6. doi: 10.25259/JORP_30_2023
Abstract
At present, ophthalmoplasty largely consists of oculofacial esthetic procedures in addition to diseases of the lid, lacrimal, orbit, and oncology. Meticulous pre-operative assessment and technically advanced surgery goes a long way in attaining patient satisfaction. Oculofacial esthetics involve both medical and surgical measures. This review includes the basics of training and setup of esthetic practice, patient selection, and evaluation before esthetic procedures. It dwells on the non-surgical and surgical aspects of commonly performed oculofacial esthetic procedures.
Keywords
Oculoplasty
Oculofacial esthetics
Aging face
Blepharoplasty
Face-lift

INTRODUCTION
An ophthalmic plastic surgeon most commonly deals with lacrimal conditions, orbital surgeries, and ocular oncology. However, along with eyelid procedures, more and more oculoplastic surgeons are opting to practice esthetics. Now that the periocular region has come into focus from an esthetics perspective, it is imperative that practicing oculoplastic surgeons equip themselves with the know-how to manage these patients. It is also important to create awareness among the general public that as surgeons, we are well equipped to handle eye related as well as most facial procedures safely.
PARADIGM SHIFT
Esthetic treatments are not only limited to the aging face, namely, “face-lifts” that were traditionally performed by plastic surgeons, but are also open to the younger population to enhance their facial features or correct any preexisting undesirable flaws. Another paradigm shift has been that of patients opting for less and less invasive procedures rather than “going under the knife”. The global survey done by the International Society of Aesthetic Plastic Surgery in December 2020 shows that face and head procedures have increased by 14.5%, with men increasingly opting of esthetic surgeries.[1] India has one of the largest groups of oculoplastic surgeons in the world and is now ranked within the top 10 countries where esthetic procedures are being performed.[1]
TRAINING
Oculofacial procedures must be done by a qualified surgeon after completing training in either ophthalmic plastic surgery or training pertinent to any other surgical field. Improper methods or untrained surgeons performing these techniques may result in complications and lead to litigation. In our country, there are various institutes that conduct fellowships and short-term instruction courses in esthetic procedures. International observerships and fellowship programs such as those offered by the International Council of Ophthalmology give candidates an opportunity to learn from reputed colleges and mentors.
SET-UP
To start in the journey of providing esthetic and cosmetic services to the patients, it is important to modify practice to cater the clientele. It is equally crucial to gain confidence of the subject in the result of these procedures. Moreover, to do the same, efficient scheduling and well-informed communications by doctors and counselors are very important. The design of the clinic should be appealing and comforting to the patients. In today’s time, where patients do a lot of research before choosing a particular doctor, social media handles of the clinic should have appropriate data in forms of images and videos.
ANATOMICAL CHANGES
The aging face shows changes in bone, fat and other soft tissues, facial muscles, and connective tissue. Midfacial aging is thus an interplay of several factor and a three-dimensional process that includes loss of volume, descent, and surface alterations [Figure 1].[2] Due to accelerated bony resorption, there is enlargement of orbital rim, shortening of maxilla, and decrease in the length and height of mandible.[3] There is associated deepening of nasolabial fold (NLF) and atrophic changes resulting in hollowing of cheeks. Dermal thinning, decreasing skin elasticity, and fat atrophy coupled with muscular traction and bony volume loss result in rhytids and the formation of creases, NLFs, jowls, and the aged appearance of facial skin [Figure 2].[4]
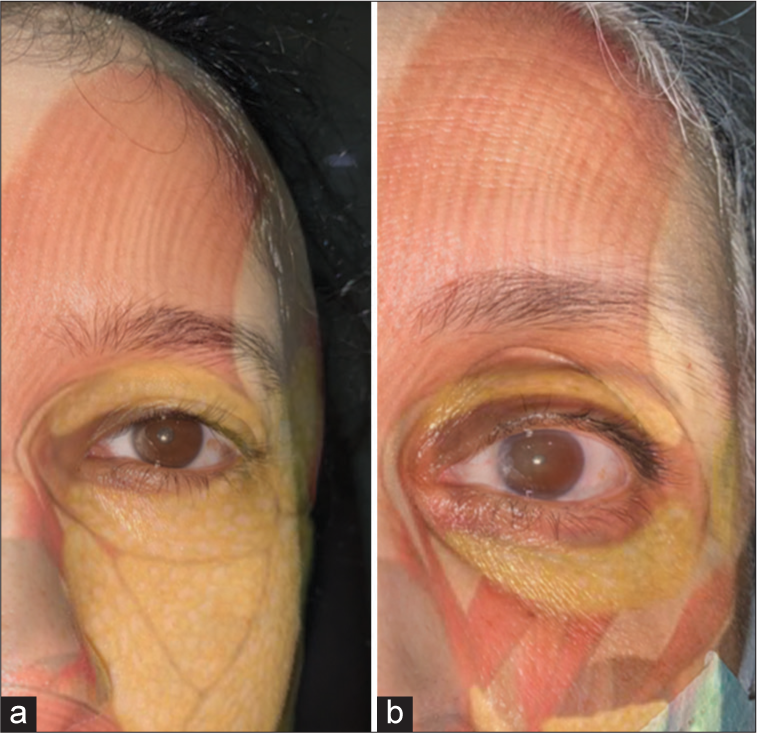
- Interplay between fat and facial muscles changing with age: (a) In a 26-year-old lady and (b) In a 65-year-old lady.

- Bony aging: (a) The maximum resorption of bone takes place in the superomedial and inferotemporal orbit. (b) This results in elevated medial aspect of the brow and lengthening of the lid-cheek junction.
PATIENT SELECTION
Deciding whether or not a patient is an ideal candidate for a procedure is of utmost importance. It is necessary to assess the patient’s expectations and proceed only once both client and doctor are on the same page. Counseling before the procedure, regarding realistic and achievable results, can make the difference between satisfied and unsatisfied patients.
Procedures should be avoided or done under caution in patients who have:
Pre-existing dry eye disease
Known bleeding or clotting disorders
Patients on antiplatelets and anticoagulants
Neuromuscular disorders
History of blepharochalasis
Unreasonable expectations.
Patient evaluation:
Skin diseases, for example, Rosacea, Acne
Facial symmetry and bone structure
Shape and position of the brow
-
Upper lid
Excess skin
Ptosis, Lid retraction
Position and symmetry of lid crease
Prolapsed orbital fat
Xanthelasma
Dermatitis
Prolapsed lacrimal glands.
-
Lower lid
Tear trough deformity/hollowness
Abnormal lid position – entropion/ectropion/lid retraction
Excess skin, rhytids
Protruding orbital fat
Eyelid laxity
Lateral canthal rounding
Hypertrophic orbicularis muscle
Malar bags or festoons.
-
Rhytids
NLF
Smoker’s lines
Marionette lines
Glabellar lines, forehead creases
Crow’s feet.
TREATMENTS
Non-surgical
Cosmeceuticals – Acne treatment, Depigmentation, Sunscreens, and Emollients
Dermabrasion - The most common indications for dermabrasion are in the treatment of acne scars, vitiligo, traumatic or surgical scars, photo damage, few benign tumors, actinic keratoses, and perioral rhytides. Furthermore, melasma, tattoos, or post-inflammatory hyperpigmentation can be lightened with dermabrasion. It gives 35–50% improvement. Patients should be told that the maximal effect is usually observed 6 months after surgery
Facial peels – They can be superficial, medium depth and deep peels, based on the indication
Laser resurfacing – By pulsed carbon dioxide and erbium: Yttrium-aluminum-garnet or combination of these two.
Botulinum toxin injections – They are used to smoothen out static and dynamic wrinkles. It is also useful in patients who have a prominent orbicularis roll below the lashes. They can also be combined in solutions used for microneedling along with hyaluronic acid as “mesobotox” to give a good glow to the skin
Filler injections – To improve scars, fine wrinkles, grooves, and folds, as well as to address periorbital hollows. Permanent fillers are polymethyl-methacrylate microsphere and silicon, their use is no longer preferred. Autologous fat, hyaluronic acid, Poly L-Lactic acids (PLLA), collagen are temporary fillers. Temporary fillers are most commonly preferred due to their safety and reversibility [Figure 3].
Thread lifts – Cogged/barbed threads are inserted under the skin and tightened by engaging soft tissue and muscle, thereby lifting tissues as well as stimulating collagen production. They can be made of Polydioxanone, PLLA, and Poly Caprolactone.

- Procedure of Hyaluronic acid injections for tear trough.
Surgical
Blepharoplasty
Upper lid blepharoplasty – To address hooding and bulging fat pads. It can be done for both functional and cosmetic purposes. Brow ptosis should be addressed before proceeding with upper lid blepharoplasty.
Achieving symmetry requires accurate measurements of skin and muscle to be excised. The marking should be done in the sitting position when the tissues are in their normal gravitational relationship. Initially, skin crease incision should be marked which is precisely at the crease in younger patients and 1 mm caudal to existing crease for older patients. The amount of skin left after excision should be at least 20 mm between eyebrow and eyelashes to ensure proper lid closure.
After skin and muscle excision, septum is identified, and it is opened throughout its length. At this point, preaponeurotic fat is seen and is dissected off the levator towards the superior orbital rim. The central and medial fat pads are excised.[5] Crease forming sutures may be passed from skin to the aponeurosis with 6-0 vicryl. Skin is closed with 6-0 prolene.
Lower lid blepharoplasty – Mainly to address fat prolapse and skin laxity. It is most commonly performed through the inferior transconjunctival approach. Transconjunctival approach is preferred in cases where there is no excess skin and muscle. Incision is given along the inferior edge of the tarsus. Septum is opened and excess fat lying anterior to the inferior orbital rim is excised or redraped as needed. Conjunctival incision is closed using 6-0 vicryl sutures.
In the transcutaneous approach, a subciliary incision is made below the lashes from the punctum up to 5 mm lateral to lateral canthus. Traction sutures are passed and dissection is carried out till the inferior orbital rim is reached. After identifying orbital septum, it is incised and the underlying fat is exposed. Excess fat from the three fat pads, namely, lateral, central, and nasal fat pads are excised. As lateral fat pad is obscured with multiple septae, it may not appear easily, necessitating dissection. The medial fat compartment is the most difficult to locate. Appearance of medial fat pad is different from lateral and central fat pads, as it is white and membranous. Judicious excision should be done, as immoderate removal of fat posterior to inferior orbital rim may be a cause of hollow look.[6] When the anterior fat border lies flush with the inferior orbital rim on pressure over globe, it indicates the end point of fat excision. Skin and muscle excision must be done conservatively as inadvertent removal may cause ectropion. Skin incision is closed with 6-0 prolene [Figure 4].
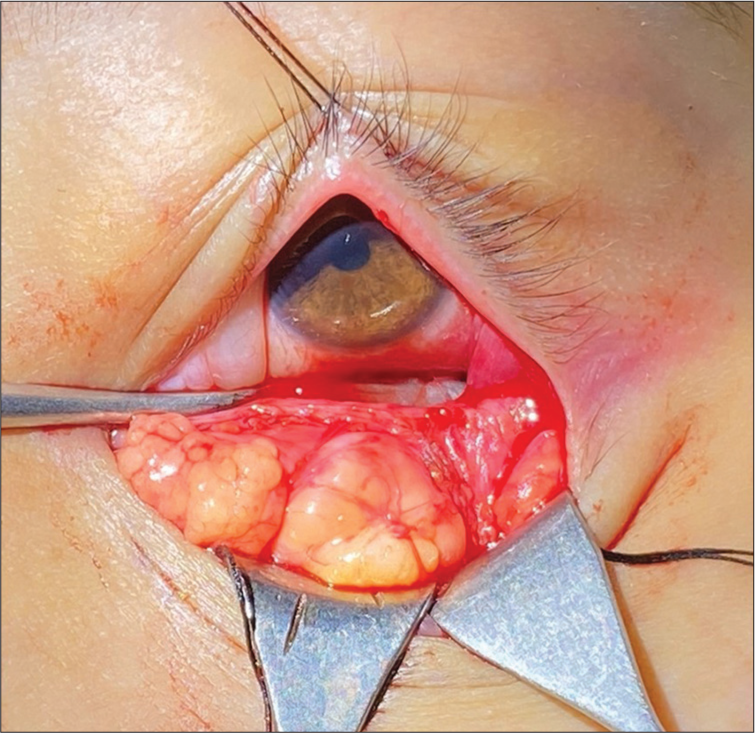
- Image showing the medial, central, and lateral fat pads dissected at the time of lower lid transconjunctival blepharoplasty.
Browplasty
It is used to correct fullness due to abundance of retroorbicularis oculi brow fat.
Brow lift
To address brow ptosis
Supra-brow lift-open (traditional) brow lift with incisions just above the eyebrows
Temporal brow lift-in the mid forehead region
Frontal brow lift-in the hairline
Coronal brow lift
The various routes are subperiosteal, subgaleal, or subcutaneous. Subgaleal approach is the most common route through a hairline or coronal incision. Pre-operative assessment and skin marking are the most crucial steps. The brow is lifted to the desired position and a ruler is positioned next to inferior brow hair. The eyebrow is allowed to drop and this distance is measured and multiplied by a factor of 1–1.5 to calculate the height of final incision. An elliptical area is marked above the eyebrow. Skin and muscle are excised in one layer. Supraorbital nerve medially and frontal nerve laterally should be preserved. Wound is closed in 2 layers with 4-0 vicryl and 6-0 non-absorbable interrupted sutures.
Endoscopic – Brow elevation may be achieved to a predictable degree, but fixation remains a concern with the endoscopic lift. Multiple techniques have been described which includes suture suspension, screw, and K-wire fixation. Endoscopic techniques, due to limited incisions, proves to be desirable to patients and considered as a “minimally invasive procedure.”[7]
Ptosis
The choice of the surgery is determined on the basis of following:
Unilateral or bilateral ptosis
Ptosis severity
Action of Levator palpebrae superioris
Any associated anomalies.
Depending on the above criteria, commonly performed procedures are:
Fasanella servat
Müller’s muscle-conjunctival resection
Levator resection
Brow suspension ptosis repair commonly known as Frontalis sling surgery.
Eyelid malpositions
Other eyelid conditions include ectropion, entropion, and lid retraction. Lid retraction can be non-surgically corrected by botulinum toxin injections. Surgically, it can be managed with a single or combination of procedures such as – retractor release, levator disinsertion, spacer grafts (e.g., Hard palate graft), and lower lid tightening.
Mid face-lift
It is also known as midface suspension and mainly aims at elevation and tightening of the soft tissues such as fat and muscle of the cheek area. It restores a more youthful lower eyelid-cheek “continuum”, by lifting the NLF and partial softening of the “tear trough deformity” and improving the appearance of the malar bags (“cheek bags”). It is usually performed under general anesthesia due to extensive dissection of facial tissues.
COMMON COMPLICATIONS OF ESTHETIC PROCEDURES
Hematoma
Infection
Eyelid retraction
Lagophthalmos
Ectropion/symblepharon
Ocular motility problems
Blindness.
CONCLUSION
A plethora of new and emerging esthetic procedures have entered the market, which are gradually being applied to ophthalmic practice with the help of oculoplastic surgeons. It is important that we learn to cross-specialize in this era, specifically with reference to dermatology as this can help surgeons to deliver holistic care to their clients.
Ethical approval
Not applicable.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
Dr. Ashok Kumar Grover is on the editorial board of the Journal.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- ISAPS Global Survey. 2020. Available from: https://www.isaps.org/discover/about-isaps/global-statistics/reports-and-press-releases/global-survey-2020-full-report-and-press-releases-english [Last accessed on 2021 Dec 28]
- [Google Scholar]
- Contemporary thoughts on lower eyelid/midface aging. Clin Plast Surg. 2015;42:1-15.
- [CrossRef] [Google Scholar]
- Changes in the facial skeleton with aging: Implications and clinical applications in facial rejuvenation. Aesth Plast Surg. 2012;36:753-60.
- [CrossRef] [PubMed] [Google Scholar]
- Facial fold and crease development: A new morphological approach and classification. Clin Anat. 2019;32:573-84.
- [CrossRef] [PubMed] [Google Scholar]
- The five-step lower blepharoplasty technique refined. Plast Reconstr Surg Glob Open. 2020;8:e2717.
- [CrossRef] [PubMed] [Google Scholar]
- The endoscopic brow lift. Atlas Oral Maxillofac Surg Clin. 2016;24:165-73.
- [CrossRef] [PubMed] [Google Scholar]




