
Translate this page into:
Tenons patch graft in management of old corneal tear – A case report

*Corresponding author: Bikram Dam, Cornea and Anterior Segment Services, Shantilal Shanghvi Cornea Institute, LVPEI, Hyderabad, Telangana, India. doctorvikramdam@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Joshi VP, Dam B. Tenons patch graft in management of old corneal tear – A case report. J Ophthalmic Res Pract. 2024;2:24-7. doi: 10.25259/JORP_37_2023
Abstract
Tenons patch graft (TPG) has been in common therapeutic use for a variety of ocular disorders. We present a case report of a 20-year-old female who presented to us with the left eye corneal perforation with cystic changes in the iris along with its prolapse managed with TPG alongside iris abscission resulting in fine integration of TPG, along with cornea and subsequent visual restoration by management of traumatic membranous cataract.
Keywords
Tenons patch graft
Corneal perforation
Iris cyst
Traumatic cataract

INTRODUCTION
Cornea, by virtue of its location, is very prone to environmental insults and is the most common site of eye injury.[1] In developing countries due to the limited availability of tertiary eye care and affordable health-care facilities, eye injuries are frequently neglected. Old corneal tears remain a potential area of weakness, subsequently leading to corneal perforations. Corneal perforations with intraocular content extrusion are associated with significant ocular morbidity and warrant urgent intervention.
Various management options have been described in the literature for globe restoration, and which encompasses from tissue adhesive to corneal transplantation depending on the location, size, contents, and causative etiology of the perforations.
The principle of using autologous tissue is beneficial due to the immunological advantages, reduced chances of graft rejection, economic advantages, and reduced dependence on eye banks in an already tissue-deficient setting. This also provides the added advantage of successful future grafts as it prevents heterogenic sensitization.[2]
Tenons patch graft (TPG) has been previously described in the literature for repairing traumatic scleral perforations and leaking trabeculectomy blebs and pterygium surgeries.[3]
Vajpayee[4] gave the first description of the use of autologous tenon’s tissue as a patch graft, that was presented as part of the of video series of the American Academy of Ophthalmology, and since then, it has been used usually for perforations of size 3–5 mm, but its use in bigger perforations[5] also finds mention in literature.
There is a dearth of available literature on the use of TPG in perforations post old neglected corneal tears and the surgical options of suturing a very fragile cornea vis-a-vis TPG and its integration in cornea and the future visual outcome.
CASE REPORT
A 20-year-old female from Maharashtra, India, presented to our department with complaints of pain, photophobia, and diminished vision in the left eye since one month. She was locally diagnosed with corneal perforation and treated with tapering doses of topical steroids, antibiotics, and pain medications.
The patient gives a history of trauma to the left eye by grass while working in the fields around two months back.
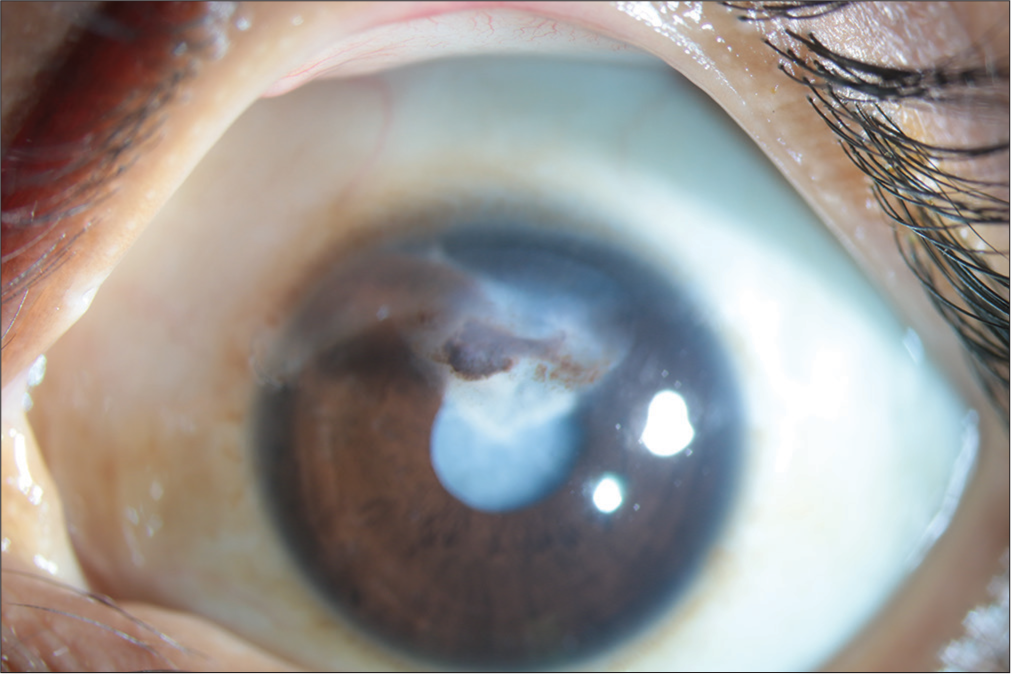
At presentation, the affected eye had the best-corrected visual acuity (BCVA) of hand movement close to face (HMCF). Slit-lamp evaluation was suggestive of a large central descemetocele with encysted iris tissue and traumatic cataract [Figure 1].
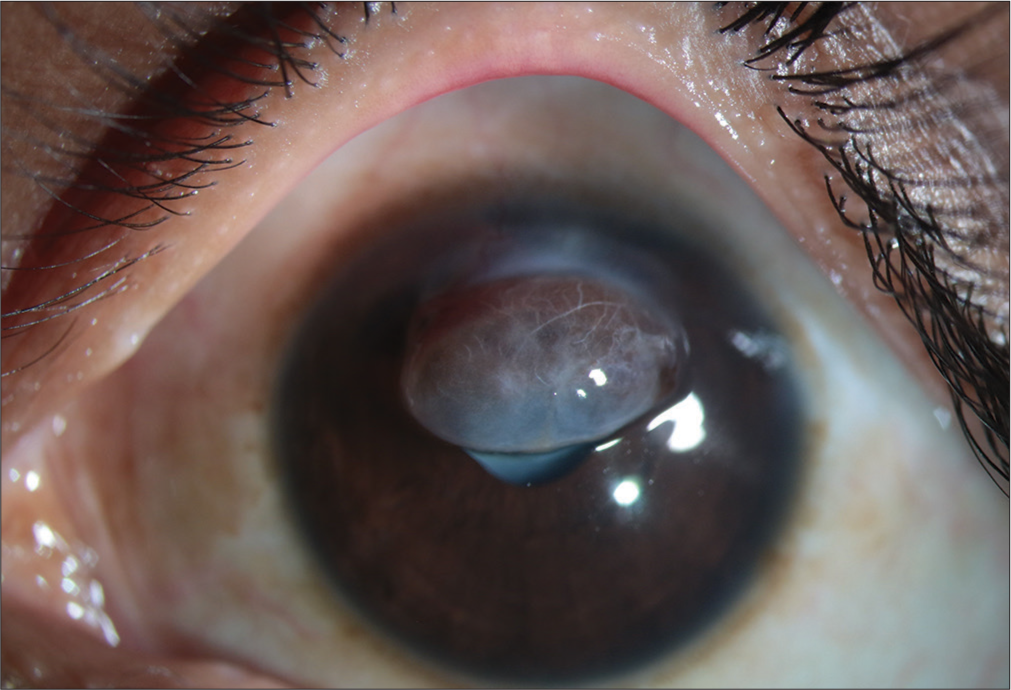
- Slit-lamp image showing a large central descemetocele with encysted iris tissue and traumatic cataract.
Anterior segment optical coherence tomography (AS-OCT) (Optovue, Fremont, CA) imaging revealed a cystic lesion of the iris [Figure 2] and B-scan ultrasonography (USG B-Scan) (accutome connect B-scan) findings were within normal limits [Figure 3].
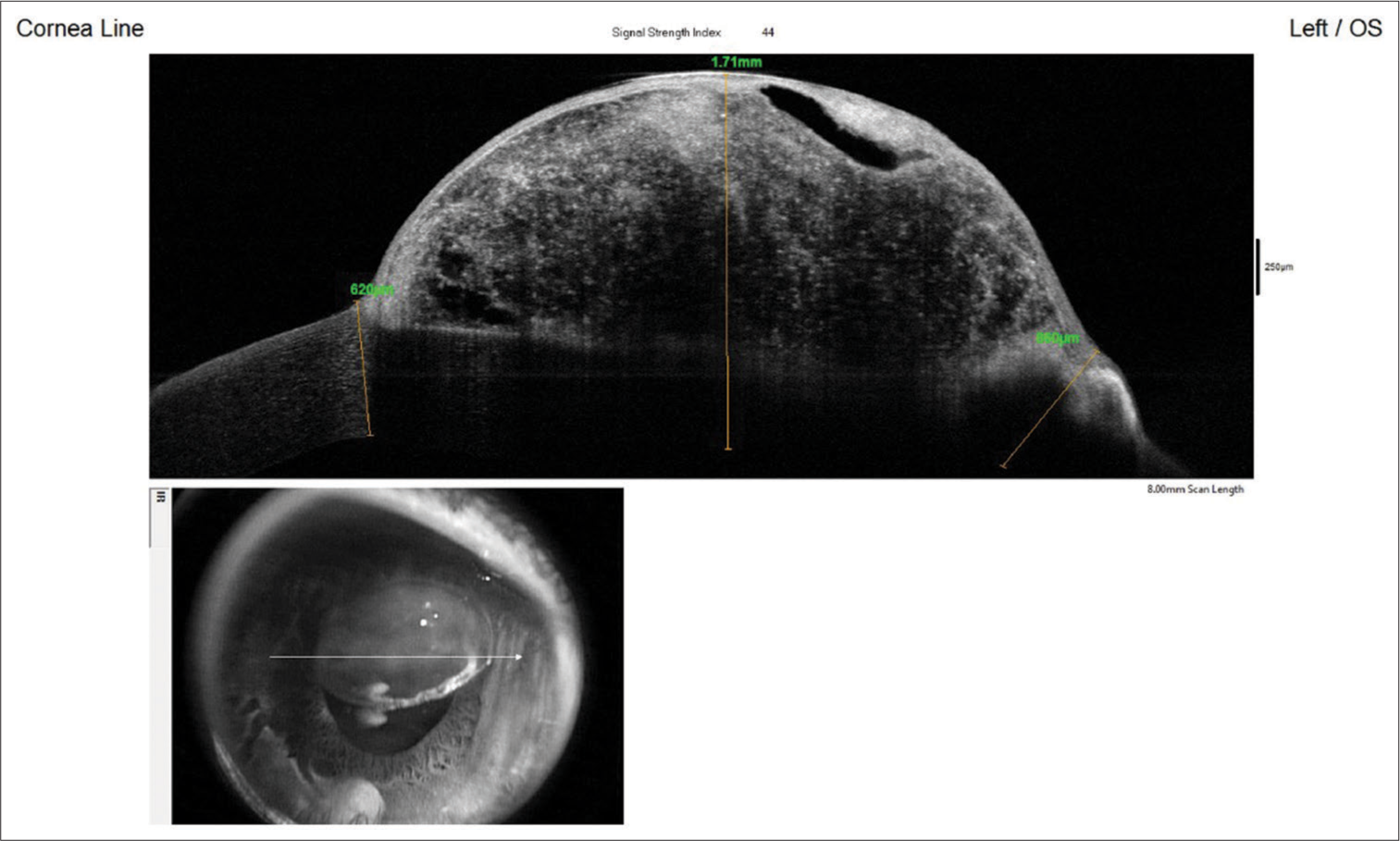
- AS-OCT - Anterior segment optical coherence tomography (Optovue, Fremont, CA) image showing cystic lesion of the iris.
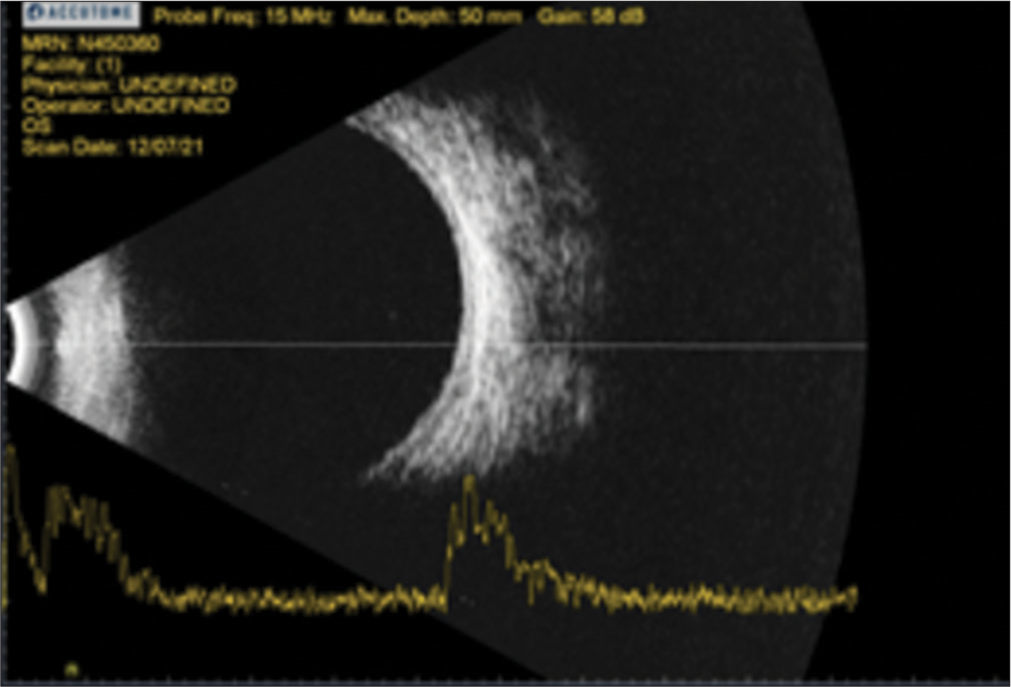
- B-scan: Brightness scan (accutome connect B-scan) findings were within normal limits.
A diagnosis of the left eye corneal perforation 5 × 3 mm (V × H) was made, and the patient was planned for a two-staged procedure with TPG/corneal patch graft with iris abscission as the primary procedure followed by lens aspiration with intraocular lens implantation for visual rehabilitation.
Intraoperatively epithelial cyst excision was done and an old corneal tear noted, wound margin was then freshened and TPG secured from the inferotemporal quadrant and tucked in the defect followed up with amniotic membrane graft (AMG) overlay and secured with Fibrin glue (Tisseel Kit, Baxter AG, Vienaa, Austria) [Figure 4]. Bandage contact lens was placed at the end of the procedure.
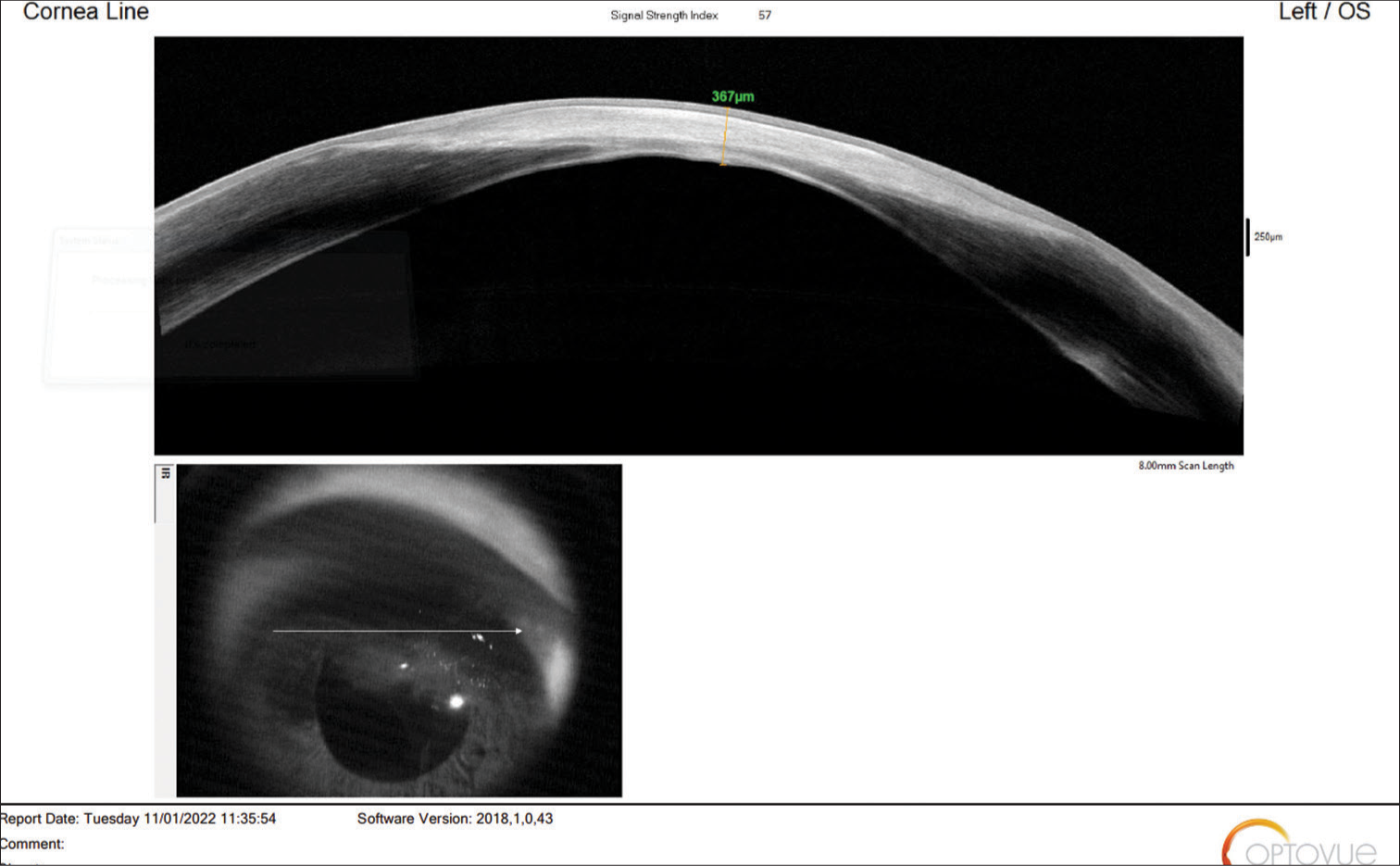
- AS-OCT - Anterior segment optical coherence tomography (Optovue, Fremont, CA) image showing fine integration of tenons patch graft in the cornea.
Postoperatively, she was prescribed prednisolone acetonide 1% six times/day, moxifloxacin 0.5% four times/day, and homatropine hydrobromide 2% thrice daily. Histopathological evaluation of the iris abscission sample was suggestive of epithelial implantation.
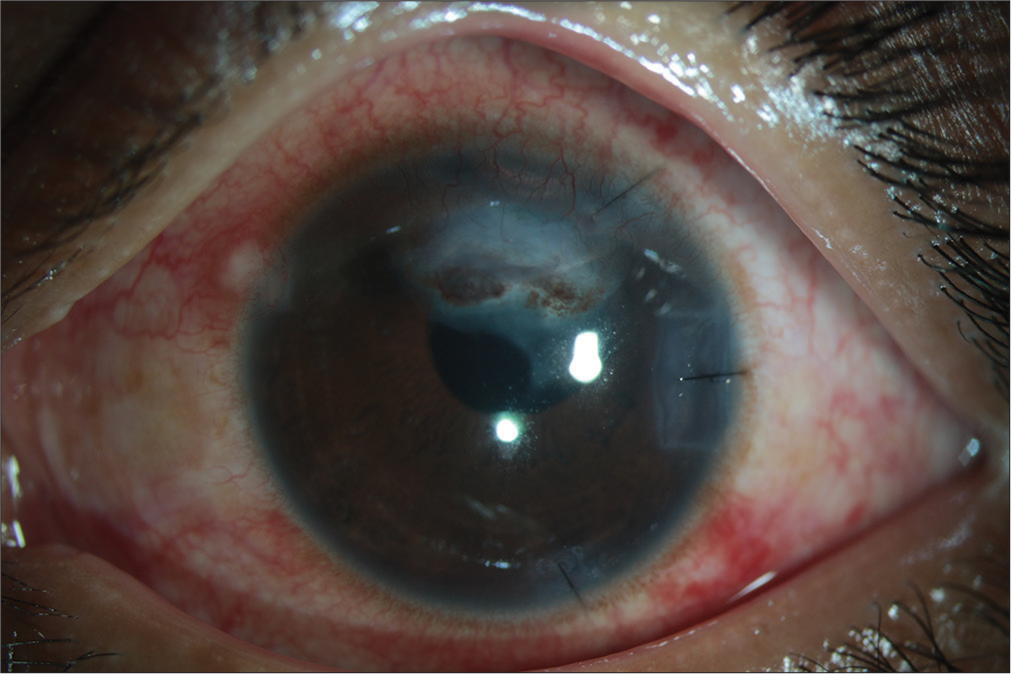
The patient was followed on day 1, day 7, and 5 months post-surgery. At 5-month follow-up, TPG was found to have healed properly with AS-OCT (Optovue, Fremont, CA), showing fine integration of TPG in the cornea where the TPG became compact, thin, and translucent; however, the BCVA was HMCF [Figure 5].
- Slit-lamp image showing healing of tenons patch graft with traumatic cataract.
The diminished vision of the patient was explained by traumatic membranous cataract with posterior synechiae, and after an uneventful lens aspiration, synechiolysis, and IOL (Single piece) placement surgery, the BCVA improved to 20/50 on post-operative day 1 and to 20/30 on post-operative day 30 [Figure 6].
- Slit-lamp image of the patient after an uneventful cataract surgery.
DISCUSSION
Various surgical techniques have been described in the literature to manage corneal perforations with successful closure. The aim of management in the case of corneal perforation due to any cause is to maintain the integrity of the globe and visual restoration if and when feasible.
Some of the common materials in use are cyanoacrylate glue, multi-layered amniotic graft, corneal patch graft, penetrating keratoplasty, lamellar graft, and temporalis fascia lata which have their own advantages and disadvantages.
The various advantages of TPG that have led to its increased popularity are its autologous nature, inexpensive, easy accessibility, effectiveness in sealing perforations, and reduced dependence on eye banks, which are a major barrier in developing countries.[6]
TPG has autologous fibroblasts, which have been seen to play a role in its incorporation into the host cornea without causing any significant scarring.[7] The successful adherence into the cornea also makes the corneal tissue withstand significant stress during the anterior segment procedure, as seen in this case.
Korah et al. did a six-year retrospective study on 28 patients who had corneal perforations of size 3–6 mm and underwent TPG and reported healing in 20 patients with the maintenance of the anterior chamber.[5]
Our case shows a successful wound closure and subsequent visual restoration in a patient presenting with cystic changes in the iris with an old neglected corneal tear where due to friability of tissues, suturing of wound margins was not feasible.
This case report will encourage more surgical interventions in old neglected corneal tears being managed with TPG.
CONCLUSION
This case demonstrates the anatomical closure and visual restoration in a patient with iris cystic changes with an old corneal tear and reasserts the tensility of TPG for subsequent anterior segment surgeries.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent is not required as the patients identity is not disclosed or compromised.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Epidemiology of eye injuries in a high-income developing country: An observational study. Medicine (Baltimore). 2019;98:e16083.
- [CrossRef] [PubMed] [Google Scholar]
- Management of corneal perforations: An update. Indian J Ophthalmol. 2020;68:7-14.
- [CrossRef] [PubMed] [Google Scholar]
- Use of autologous Tenon's capsule and scleral patch grafts for repair of excessively draining fistulas with leaking filtering blebs. J Glaucoma. 1998;7:417-9.
- [CrossRef] [PubMed] [Google Scholar]
- Tenon patch graft for corneal perforation. Available from: https://www.aao.org/annual-meeting-video/tenon-patch-graft-corneal-perforation [Last accessed on 2022 Jun 06]
- [Google Scholar]
- Tenons patch graft in the management of large corneal perforations. Cornea. 2016;35:696-9.
- [CrossRef] [PubMed] [Google Scholar]
- Tuck-in tenon patch graft in corneal perforation. Cornea. 2019;38:951-4.
- [CrossRef] [PubMed] [Google Scholar]
- Tenon patch graft for corneal fistula: A rare entity treated by a simple technique. Case Rep. 2017;2017:bcr-2017.
- [CrossRef] [PubMed] [Google Scholar]




