
Translate this page into:
Ultrasonography in ocular trauma: A pictorial description

*Corresponding author: Jessica Basumatary, Department of Medical Retina and Uvea, Sri Sankaradeva Nethralaya, Guwahati, Assam, India. jazzme6799@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Deka H, Basumatary J. Ultrasonography in ocular trauma: A pictorial description. J Ophthalmic Res Pract 2023;1:39-43.
Abstract
Ultrasonography is an indispensable diagnostic tool for examination of the eye after ocular trauma, which can be quite challenging due to various reasons like lack of patient cooperation, hazy media, and injury to periocular structures. We have retrospectively analyzed the case records of 269 patients who had sustained ocular trauma over a span of 1 year and compiled the data of the findings that were obtained from ultrasound scan. The scan was found to be normal in most cases (27.63%) and the second most common finding was retinal detachment (24.36%). Other findings that were noted are vitreous hemorrhage, choroidal detachment, optic nerve avulsion, endophthalmitis, panophthalmitis, presence of intraocular foreign body, and phthisis bulbi.
Keywords
Ultrasonography
B-scan
Ocular trauma

INTRODUCTION
The World Health Organization has estimated that blindness resulting from ocular trauma affects 1.6 million people worldwide annually and the prevalence of ocular trauma is 2–6%.[1]
In ocular traumas associated with facial injuries, the incidence of visual loss and blindness is as high as 10.8% and 84% of patients with head injuries have ocular injuries.[2]
Examination of the globe is difficult after a trauma. The presence of periorbital swelling and other injuries pose difficulties during the examination along with factors like poor patient cooperation. In such situations, ultrasonography (USG) as a diagnostic tool is frequently utilized.
Conventional USG has a probe that oscillates between 7.5 and 12 megahertz. It employs a unidirectional, amplitude modulated, A-scan which was first reported in 1956 by Mundt and Hughes, thereafter the two-dimensional brightness scan, that is, the B-scan was introduced by Baum and Greenwood in 1958. The two scans complement each other and are frequently used together. In open globe injuries, USG should ideally be done after the primary repair; however, if performed before the repair, it should be done with caution to minimize additional trauma and the probe should be sterilized or placed in sterile rubber sleeves. Using the immersion or water bath technique, anterior segment abnormalities can also be detected.[3]
To highlight the importance of USG in ocular trauma, a retrospective analysis of electronic medical records of all patients who presented to the emergency clinic with ocular trauma and underwent ultrasonographic examination of the eye from January 2020 to December 2020 were reviewed.
RESULTS
A total of 275 eyes of 269 patients were studied. Patients were aged between 9 months and 82 years. Mean age ± standard deviation was: 25.16 ± 19.06 years. [Figure 1] shows the different findings on B-scan in ocular trauma.
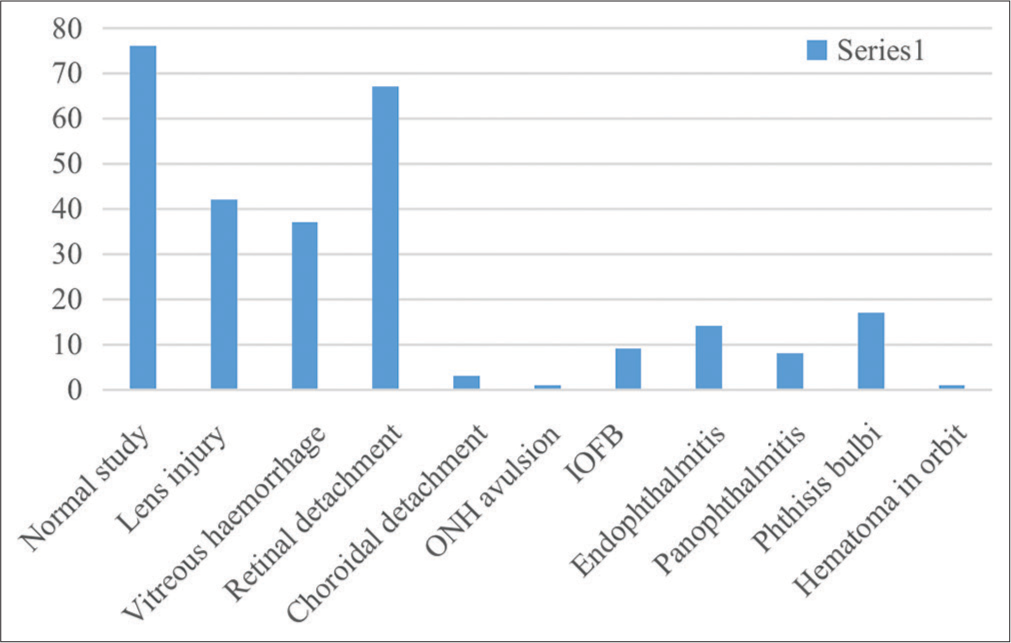
- Findings on B-scan in ocular trauma.
USG performed on the 275 eyes, showed a normal study in most cases 27.63% (n = 76), followed by retinal detachment in 24.36% (n = 67). Lens injury was seen in 15.27 % (n = 42) and vitreous hemorrhage in 13.45 % (n = 37). 6.18% (n = 17) of eyes had phthisical changes on B-scan and endophthalmitis and panophthalmitis were seen in 5.09% (n = 14) and 2.90% (n = 8) of eyes respectively. Intraocular foreign body was found in 3.27% (n = 9) of cases, one case had foreign body lodged in the lens which was detected on ultrasound biomicroscopy (UBM) examination. Choroidal detachment was seen in 1.09% (n = 3) of cases and optic nerve avulsion was seen in one case 0.36%.
LENS INJURY
It is important to know the presence or absence of the lens, its position, and integrity following a trauma. USG can detect a posteriorly dislocated lens but a subluxated lens is more clearly seen in a UBM scan[3] [Figure 2].

- Posteriorly dislocated lens in vitreous cavity.
VITREOUS HEMORRHAGE
Vitreous hemorrhage is one of the most common findings in patients with ocular trauma. Echo reflectivity may vary from low to high. Kinetic scan shows an undulating after-movement which usually allows the posterior vitreous detachment (PVD) associated with vitreous hemorrhage to be differentiated from the less mobile retinal and choroidal detachments. Transverse scan of the inferior retina may show layering of the hemorrhage in long standing cases giving the appearance of pseudomembrane formations. Ultrasonographically detected vitreous band may be an indirect sign of vitreous incarceration at a perforation site[3] [Figure 3].

- Vitreous haemorrhage.
RETINAL DETACHMENT
The detached retina appears as a bright, continuous and smooth membrane of high reflectivity. In total retinal detachment, the retina has a typical triangular shape with insertion into the optic disc whereas a tractional retinal detachment has a tented or tabletop configuration. Retinal tears can be detected as tractions in the peripheral retina and dialysis can be detected in longitudinal scans by noting the disinsertion of peripheral retina from the ora serrata[3] [Figures 4 and 5].

- Tractional retinal detachment.

- Total retinal detachment.
CHOROIDAL DETACHMENT
It appears as a smooth, thick, and dome shaped membrane in the periphery with little after-movement. On A-scan, a steep rise of 100% reflectivity is produced, which on low gain has a double peak. When a 360° choroidal detachment is imaged with a transverse scan, multiple elevations producing a scalloped appearance is seen which appears to be touching each other; hence, the term “kissing choroid” is used. In cases of massive suprachoroidal hemorrhage, serial USG follow-up is important to determine the timing for surgical intervention[3] [Figure 6].

- Choroidal detachment.
Intraocular foreign body: Metallic foreign bodies produce an echo dense signal of 100% reflectivity that persists in low gain with marked shadowing of the ocular and orbital structures just posterior to it. When the sound waves pass through a spherical metallic foreign body, a portion of the wave reverberates within the object. Wood and other vegetative matter can produce various echographic findings depending on their size and density and air bubbles may produce echograms that are similar to those of true intraocular foreign bodies. Immersion technique may be necessary to detect the foreign body in the anterior segment, especially if it is located in the lens[3] [Figure 7].

- Intraocular foreign body.
Endophthalmitis: It appears as multiple echoes of low to moderate reflectivity which can be membranous, dot or clump like. In the presence of a PVD, the sub-vitreal space should be carefully examined for the presence of echoes which suggests active inflammation. Other associated findings are increased retinochoroidal thickening and tractional/exudative retinal detachments. Serial B-scan is essential to monitor the treatment and sometimes to differentiate it from post-operative toxic anterior segment syndrome (TASS) [Figure 8].[3]

- Endophthalmitis.
PANOPHTHALMITIS
It appears as diffuse thickening of the sclera and the retinochoroidal layer along with episcleral infiltration and edema, the collection of this edema in the peripapillary area gives the appearance of the classic “T-sign”[3] [Figure 9].

- Panophthalmitis.
OPTIC NERVE AVULSION
Avulsion of the optic nerve on B-scan may show an actual break in the sclera near the optic disc and the retrobulbar optic nerve may appear enlarged. In longstanding cases, a proliferative membrane may develop at the disc and the optic nerve insertion at the globe may appear atypical[3] [Figures 10 and 11].

- Optic nerve avulsion.

- Hemorrhage around the avulsed optic nerve.
PHTHISIS BULBI
The appearance of phthisis bulbi on B-scan is very characteristic. There is gross reduction in axial length of the eyeball when compared to the fellow eye, thickening of the retinochoroidal layer and loss of integrity of the intraocular structures are seen. High reflective echoes suggestive of calcification can be noted on the ocular coats[3] [Figure 12].

- Phthisis bulbi.
ORBITAL USG
Using periocular and transocular approaches, a three-dimensional scan of the orbit can be obtained on B-scan. The gain of the instrument should be reduced to visualize the echoes from deeper orbital structures. Following trauma, USG can be employed to detect injuries of the orbital tissues and extraocular muscle complex[3] [Figure 13]. Orbital B-scan performed in one case showed the presence of hematoma in superior muscle complex 0.36%.

- Orbital B-scan showing hematoma in the superior muscle complex.
CONCLUSION
USG is an important tool in assessing the globe after ocular trauma when other methods of examination are difficult to perform. It is a non-contact procedure, the USG probe can be easily placed over the closed eyelids of a traumatized eye making the procedure tolerable for the patients while providing accurate and reliable diagnostic aid. Through this article, we would like to highlight how USG has the potential to be employed as a tool to estimate the visual outcomes of patients after ocular trauma.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Gender differences in etiology and outcome of open globe injuries. J Trauma. 2005;59:175-8.
- [CrossRef] [PubMed] [Google Scholar]
- Ocular injuries in patients with major trauma. Emerg Med J. 2006;23:915-7.
- [CrossRef] [PubMed] [Google Scholar]




