
Translate this page into:
Unexpected guest

*Corresponding author: Syeda Ayesha Afreen, Department of Ophthalmology, Bangalore Medical College and Research Institute, Bengaluru, Karnataka, India. ayeshaafreen2580@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Afreen SA, Patil SS, James TM. Unexpected guest. J Ophthalmic Res Pract. doi: 10.25259/JORP_40_2024
Abstract
A 24-year-old male presented with a painful, progressively enlarging swelling in the right eye of a 2-week duration. Ocular examination revealed conjunctival congestion with a tense, tender swelling in the superonasal conjunctiva. Visual acuity remained unaffected, and no signs of trauma or systemic symptoms such as headache or seizures were noted. A biopsy after complete excision confirmed the diagnosis of cysticercosis. Postoperative treatment included albendazole and steroids. Follow-up after 1 month showed no recurrence or residual symptoms. This case underscores the importance of early diagnosis and appropriate management of ocular cysticercosis to prevent complications.
Keywords
Conjunctival swelling
Cyst excision
Histopathological diagnosis
Ocular cysticercosis

INTRODUCTION
Cysticercosis, caused by the larval form of Taenia solium (pork tapeworm), is a significant parasitic infection, especially in regions where the parasite is endemic.[1,2] While it primarily affects the central nervous system, muscles, and subcutaneous tissues, ocular involvement is a rare but potentially sight-threatening condition.[3] Ocular cysticercosis can manifest in various ocular structures, including the conjunctiva, orbit, retina, and vitreous, depending on the site of larval encystment.[4] The clinical presentation can range from asymptomatic to severe visual impairment, making early diagnosis and intervention crucial.[1]
Conjunctival cysticercosis is uncommon, and its non-specific clinical signs, such as swelling or congestion, can easily be misdiagnosed as other more common ocular conditions.[2] Failure to identify and treat the infection promptly can lead to complications such as inflammation, scarring, or even vision loss.[3] This report presents a rare case of conjunctival cysticercosis in a young adult male, discussing the clinical presentation, diagnostic process, treatment, and successful postoperative outcome. The case highlights the importance of considering parasitic infections in the differential diagnosis of ocular swellings, particularly in endemic regions.[4]
CASE REPORT
A 24-year-old male presented to our clinic with complaints of swelling in the right eye, which had developed suddenly 2 weeks prior [Figure 1]. The swelling was gradually progressive and associated with localized pain but was not accompanied by discharge, diplopia, or diminution of vision. The patient denied any history of trauma or previous ocular surgery, as well as any systemic symptoms such as seizures, vomiting, or headache.
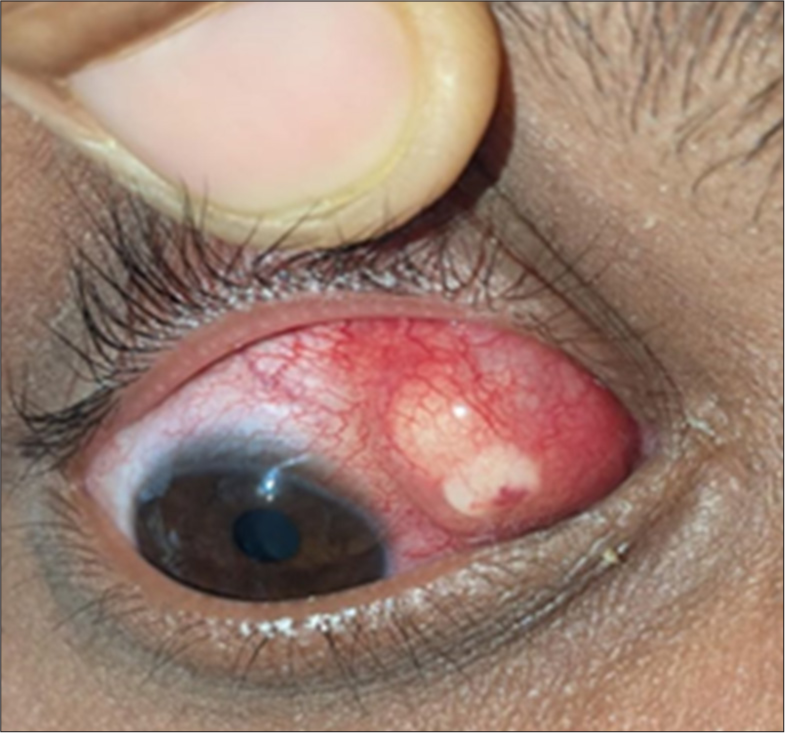
- A 24-year-old male with swelling in the superonasal quadrant of bulbar conjunctiva in right eye showing marked inflammation.
On examination, the patient’s visual acuity was 6/6 bilaterally. The lids were normal, and there was conjunctival congestion with a 6 × 5 mm tense, tender swelling in the superonasal conjunctiva of the right eye. The swelling was firm and nonfluctuant, and the overlying conjunctiva appeared congested but intact. The cornea was clear, and the anterior chamber contained optically clear content. The pupil was round, regular, 3 mm in size, and reactive to light. The lens was clear, and no abnormalities were detected in the posterior segment. Mild restriction of ocular motility was noted superiorly and medially.
Given the clinical findings, differential diagnoses included a conjunctival abscess and an infective lesion. To confirm the diagnosis, we performed a complete in-toto excision of the cyst [Figure 2a]. Intraoperatively, the cyst measured approximately 3 mm × 3 mm and had a transilluminate wall with a white, chalky material visible inside [Figure 2b].
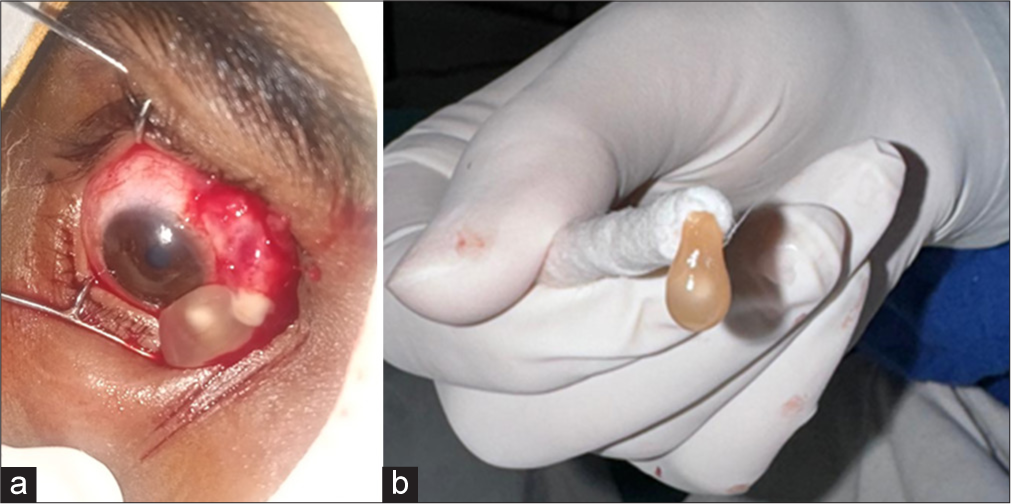
- (a) Intraoperative photograph depicting fluid-filled cyst with white chalky material. (b) In toto excised cyst.
Histopathological examination of the excised tissue revealed granulation tissue with dense inflammatory cell infiltrate consisting of eosinophils, lymphocytes, neutrophils, and histiocytes [Figure 3a]. In addition, an irregularly shaped eosinophilic thick membrane of a parasite with the presence of a scolex was identified, confirming the diagnosis of conjunctival cysticercosis [Figure 3b].
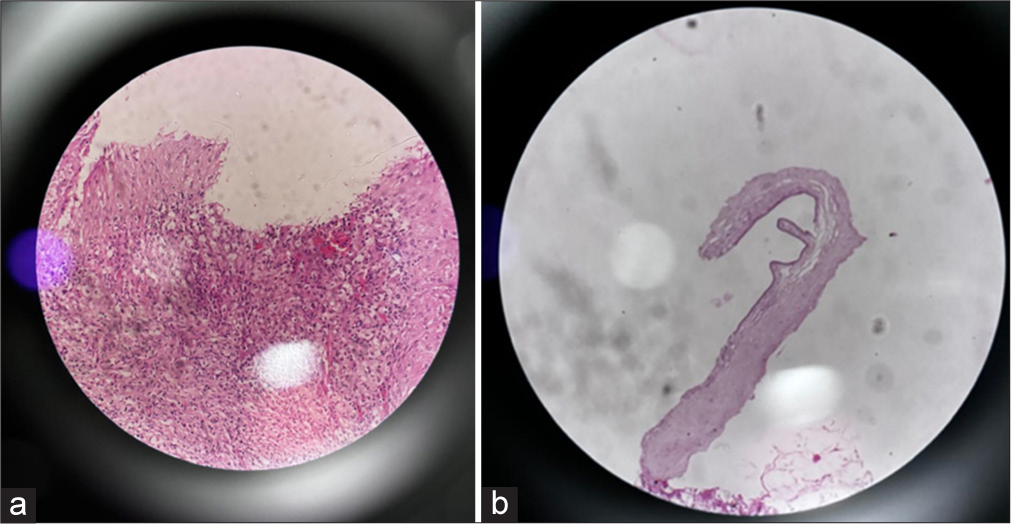
- (a) Histopathological examination of excised tissue depicts dense inflammatory cells infiltrated with abundant eosinophils (Hematoxylin and eosin stain, ×100). (b) Picture depicting cysticercosis larva.
Postoperatively, a B scan was performed to check for the presence of a cyst, but none was detected. The patient was evaluated by a neurologist, and computed tomography of the brain and orbit was done to rule out neurocysticercosis. The patient did not have any other cysts. The patient was prescribed albendazole 15 mg/kg/day for 4 weeks and corticosteroids (prednisolone) at a dose of 1 mg/kg body weight per day, tapering over the course of 1 month. The corticosteroids were administered to reduce inflammation and prevent a severe inflammatory response from the dying larva.
At 1-month follow-up, the patient reported complete resolution of symptoms. Visual acuity remained 6/6, and there was no evidence of recurrence or residual swelling. The conjunctiva appeared normal, with no signs of congestion or scarring. The patient was advised to continue regular follow-up, but no further intervention was required.
DISCUSSION
Ocular cysticercosis, though rare, is a significant condition due to its potential for severe visual impairment if left untreated.[3] It occurs when the larvae of T. solium infect the eye, most commonly affecting structures such as the subretinal space, vitreous cavity, and conjunctiva.[1] Cysticercosis of the conjunctiva is a less common manifestation but can be easily misdiagnosed due to its non-specific presentation.[4] The embryo hatched out of the egg penetrates the stomach wall and enters the blood. It reaches the orbit through the ophthalmic artery and posterior segment through choriocapillaris and reaches the subretinal space.[5]
Diagnosis is often clinical, supported by imaging modalities such as ultrasonography or computed tomography. However, a definitive diagnosis is achieved through histopathological examination.[3] Early surgical excision of the cyst is crucial not only for diagnostic confirmation but also for preventing complications such as inflammation, scarring, or secondary infections.[2]
Albendazole is the treatment of choice for cysticercosis, as it is effective in killing the parasite.[6] However, the death of the larva can trigger a significant inflammatory response, necessitating the use of corticosteroids to mitigate the associated tissue damage.[7] Therefore, it is mandatory to rule out intraocular cysticercosis and neurocysticercosis. In such cases, albendazole is delayed and corticosteroid initiated to minimize inflammation from cyst lysis.[6] In this case, the patient responded well to the prescribed regimen, and there was no recurrence of symptoms or complications during follow-up.
CONCLUSION
This case emphasizes the importance of early diagnosis and the role of combined medical and surgical management in ocular cysticercosis. Timely treatment helps in preventing complications and ensures favorable outcomes. Regular follow-up remains essential to monitor for potential recurrence and manage any long-term consequences of the infection.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Ocular cysticercosis: A clinical evaluation of 127 cases. Am J Ophthalmol. 2001;131:256-61.
- [Google Scholar]
- Conjunctival cysticercosis: A rare case presentation. Br J Ophthalmol. 1998;82:260-2.
- [Google Scholar]
- Anterior chamber cysticercosis: Management and outcomes. J Cataract Refract Surg. 2003;29:1086-91.
- [Google Scholar]
- Parasitosis in the eye: A comprehensive review. Ann Trop Med Parasitol. 2010;104:623-9.
- [Google Scholar]
- Role of steroid therapy in ocular cysticercosis treatment. Indian J Ophthalmol. 2012;60:45-9.
- [Google Scholar]




