
Translate this page into:
CM T flex scleral fixated intraocular lens short-term outcomes in different clinical scenarios

*Corresponding author: Amit S. Nene, Department of Vitreo-Retina, Isha Netralaya, Kalyan, Maharashtra, India. amitnene9@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nene AS, Patel M, Pirdankar OH, Shah S, Badole P, Shenoy P. CM T flex scleral fixated intraocular lens short-term outcomes in different clinical scenarios. J Ophthalmic Res Pract. 2024;2:9-14. doi: 10.25259/JORP_13_2024
Abstract
Objective:
The purpose is to report the visual outcomes of a “T”-shaped haptic scleral fixated intraocular lens (SFIOL) implanted using the sutureless technique in different clinical scenarios.
Material and Methods:
A retrospective case series, where patients implanted with “T”-shaped haptic SFIOL between September 2022 and February 2023, were included in the study. Subjects with missing data were excluded from the study. All surgeries were performed by a single surgeon. Pre- and post-surgery follow-up visual acuity and intraocular pressure were noted. Post-operative centration of intraocular lens (IOL), haptics condition, and occurrence of any complication were noted.
Results:
Overall, 20 eyes of 19 patients were implanted with “T”-shaped haptic SFIOL and had a mean age of 54.15 ± 15.99 years. None of the patients had any intraoperative IOL damage or any other intraoperative complication. There was a significant improvement in visual acuity post-SFIOL implantation (Paired t-test, P < 0.001), which was noted. Corneal edema was noted in one patient. IOL was stable and well-centered in all patients. No haptic-related complications were encountered.
Conclusions:
SFIOL with “T”-shaped haptic is a viable option for aphakic cases with inadequate capsular support. IOL implantation with “T”-shaped haptic is sutureless, less damaging to ocular structures and has a shorter learning curve making it easier for implantation.
Keywords
Scleral fixated intraocular lens
Visual outcomes
Aphakia
Sutureless technique
CM T Flex IOL

INTRODUCTION
Scleral-fixated intraocular lens (SFIOL) can be considered when in-the-bag intraocular lens (IOL) implantation is not feasible due to the limited support to the capsular bag as seen in cases of ocular trauma, aphakia, complicated cataract surgery, or dislocated lens such as Marfan syndrome, homocystinuria, Ehlers-Danlos Syndrome, and Congenital Aniridia.[1-4] Previous researches have described the surgical outcomes of SFIOL implanted by various techniques.[5,6]
Initially, SFIOL was implanted using a sutured technique at the expense of suture disintegration, exposure, and inflammation.[7,8] To avoid these complications, the sutureless scleral fixation technique was introduced by Gabor and Pavlidis in 2007.[1] Narang and Agarwal’s SFIOL glued technique,[3] Yamane’s double flanged technique,[2] Y fixation technique,[9] and Baskaran X-Nit technique[4] are also commonly used for SFIOL implantation. However, these techniques have a risk of intraoperative haptic breakage, haptic exposure, and IOL tilt or dislocation.[10-12]
The CM T flex is a hydrophilic, SFIOL devised to be implanted without sutures. The IOL can be implanted through an injector and has T-shaped haptics, which are placed in the scleral pockets.[13,14] To the best of our knowledge, there is limited literature describing the visual and surgical outcomes of CM T flex IOL.[13,14] The aim of this retrospective study is to describe the outcomes of “T”-shaped haptic SFIOL implanted using the sutureless technique in different clinical scenarios.
MATERIAL AND METHODS
A retrospective case series, where patients implanted with “T”-shaped haptic SFIOL between September 2022 and February 2023, were included in the study. The study was approved and reviewed by the Institutional Ethics Committee and adhered to the tenets of the Declaration of Helsinki. Subjects with missing data were excluded from the study.
Pre-operative workup included best-corrected visual acuity, intraocular pressure (IOP), and ocular biometry using IOL Master 700 (Carl Zeiss Meditech, Inc., Dublin, CA, USA) to measure axial length. IOL power calculations were performed using Sanders-Retzlaff-Kraff theoretic (SRK/T) formula and a constant of 118.0 with target refraction of emmetropia.
CM T flex is an SFIOL [Figure 1] made up of hydrophilic material with a water content of 26% and a refractive index of 1.460. The overall diameter is 13.75 mm, with an optic diameter of 6.00 mm. The angulation of the IOL is 10°.

- The design of the CM T flex intraocular lens.
All surgeries were performed by a single surgeon. Under local anesthesia, 0–180 axis marking was done to ensure centration and torsional stability of the IOL. On either side of the marking, the patient underwent conjunctival peritomy followed by cauterization, and two partial thickness scleral flaps of 2.5 mm × 2.5 mm were created [Figure 2a]. Sclerotomies under the scleral flaps were made using a 23 Gauge micro-vitreoretinal (MVR) blade.
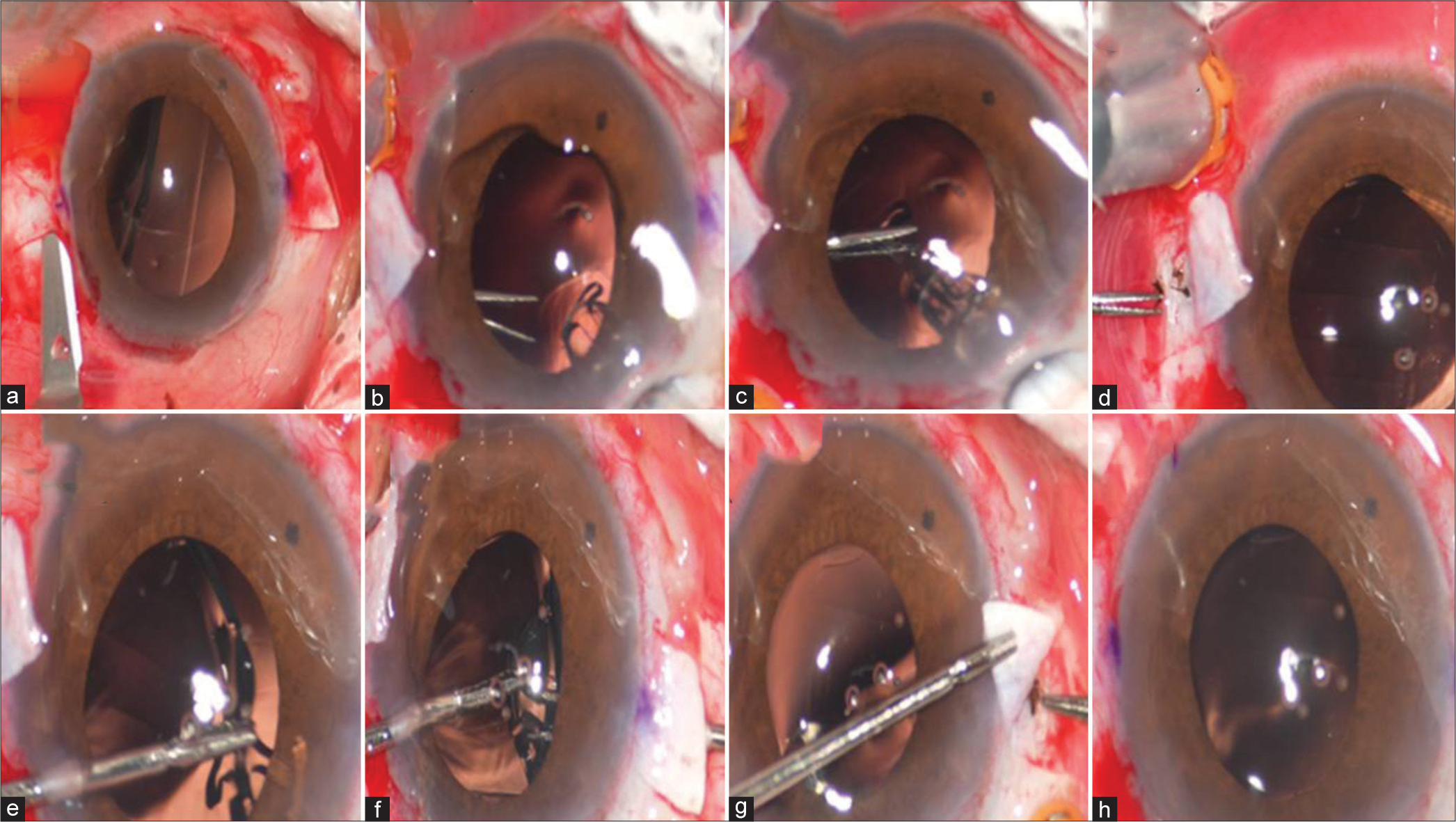
- (a) Creation of scleral flap, (b) Insertion of IOL, (c) Grasping the neck of “T” shape haptic, (d) Explantation of the leading haptic through the sclerotomy, (e-g) Using handshake technique at the other end of the haptic grasped, (h) explantation of the trailing haptic through second sclerotomy site.
A clear corneal incision of 3.2 mm was made, followed by 23 G pars plana vitrectomy. The CM T flex IOL was loaded in a butterfly cartridge and injected into the anterior chamber such that the T junction of the IOL enters first [Figure 2b]. The neck of the “T” haptic was grasped with 23 G serrated forceps [Figure 2c] and was gradually brought out through the sclerotomy [Figure 2d]. Now using another 23G forceps through the side port, the arm of the IOL was grasped [Figure 2e] and, by handshake technique [Figure 2f], was brought out through the second sclerotomy site [Figure 2g]. Fibrin glue was used to seal the scleral pockets and conjunctiva. The side port and main tunnel were hydrated. [Figure 2h] shows the well-centered IOL. The surgical steps are demonstrated in Video 1.
Video 1:
Video 1:Surgical steps demonstrating the implantation of scleral fixated IOL.The following data were retrieved for each patient before surgery and 90 days ± 30 days post-surgery follow-up: pre- and post-operative visual acuity, pre- and post-operative IOP, centration of IOL, haptics condition, and occurrence of any intra- or post-operative complication, if any.
All data were entered in Microsoft Excel and were analyzed using Minitab software. The mean and standard deviation (SD) were calculated for continuous variables and proportions for the categorical variables. Descriptive statistics were performed for all the variables. Paired t-test was carried out to compare the difference between continuous variables. Chi-square goodness-of-fit was used to evaluate the difference between categorical variables.
RESULTS
Overall, 20 eyes of 19 patients with a mean age of 54.15 ± 15.99 years were included in the study. There were eight females and 11 males. Out of 20, two had nucleus drop, seven had dislocated IOL, three had subluxated IOL, seven were aphakic, and one had Marfan syndrome. Fifteen eyes had no associated ocular pathology; however, two eyes had amblyopia, and one eye each was associated with corneal decompensation, post-endophthalmitis, and macular hole. Twelve were left eyes, whereas eight were right eyes. [Table 1] describes the baseline characteristics of patients undergoing SFIOL.
| Parameters | ||
|---|---|---|
| No of eyes. | 20 | |
| Age (years) | Mean±SD | 54.15±15.99 |
| Range | (12–74) | |
| Eyes | Right | 8 |
| Left | 12 | |
| Gender | Male | 11 |
| Female | 8 | |
| Causes | Nucleus drop, | 2 |
| Dislocated IOL, | 7 | |
| Subluxated IOL, | 3 | |
| Aphakic, | 7 | |
| Marfans syndrome | 1 | |
| Pre-surgery ocular comorbidity | Amblyopia | 2 |
| Corneal decompensation | 1 | |
| Post endophthalmitis | 1 | |
| Macular Hole | 1 | |
| Visual acuity | (Mean±SD) | 1.62±0.51 |
| IOP | (Mean±SD) | 17.10±2.79 |
IOP: Intraocular pressure, IOL: Intraocular lens, SD: Standard deviation, SFIOL: Scleral-fixated intraocular lens
In the initial two cases, difficulty was noted during grasping of T-shaped haptic and it slipped from the 23 G serrated forceps, resulting in IOL drop. The IOL was then re-grasped and the procedure completed. However, none of the patient had any intraoperative IOL damage or any other intraoperative complication.
The pre- and post-operative mean ± SD best corrected visual acuity (BCVA) was 1.62 ± 0.51 and 0.48 ± 0.59 logMAR, respectively. There was a significant improvement in visual acuity post-SFIOL implantation (paired t-test, P < 0.001).
The mean ± SD spherical equivalent refractive error was −0.70 ± 1.18 D. [Figure 3] describes the distribution of post-operative refractive error. The pre- and post-operative mean ± SD IOP was 17.10 ± 2.79 and 17.90 ± 3.41 mmHg, respectively (Paired t-test, P = 0.17).
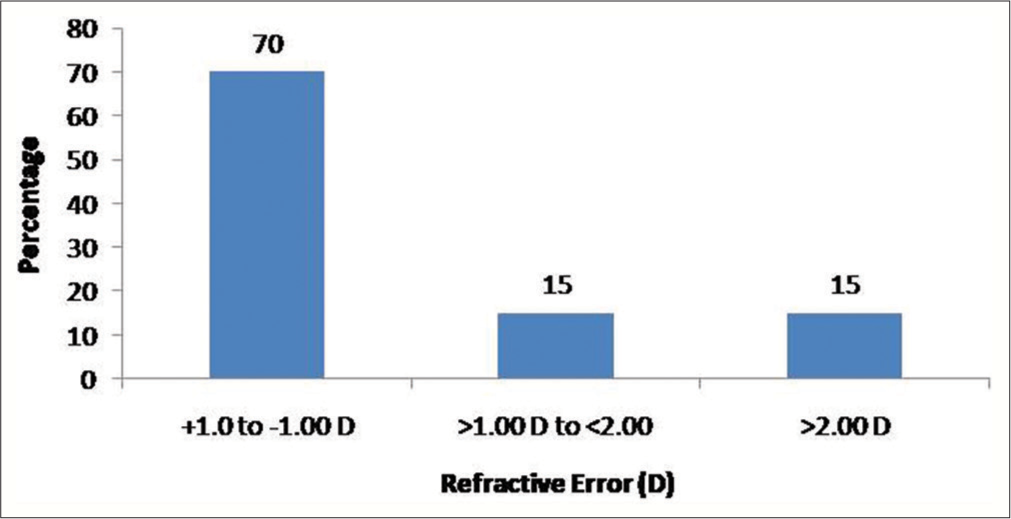
- The distribution of refractive error.
Corneal edema was noted in one patient. IOL was stable and well-centered in all patients. No haptic-related complications were encountered. One patient had post-operative choroidals, whereas two had dispersed vitreous hemorrhage all of which resolved with conservative management. No retinal complications were noted.
DISCUSSION
In patients with aphakia or inadequate capsular support, SFIOL implantation is preferred. The options available are anterior chamber IOL (AC IOL), iris-fixated IOL, and SFIOL. AC IOL can lead to complications such as corneal endothelial decompensation, secondary glaucoma, uveitis-glaucoma, and hyphema syndrome.[15,16] Iris claw lens which can be implanted in the anterior chamber or the retropupillary plane have potential to damage the endothelial cells and could result in cystoid macular edema.[17-19] Sutured SFIOL can be associated with a high risk of knot erosion which may result in endophthalmitis.[20] To avoid suture-related complications, sutureless scleral fixation with three-piece IOL was introduced. However, it may lead to haptic exposure and IOL dislocation in the long term.[6] Thus, a single-piece foldable IOL with a “T”-shaped haptic was introduced, which resulted in better visual and surgical outcomes.[14] In the present case series, we have reported the visual- and surgery-related complications of CM T flex IOL with “T”-shaped haptics.
Significant visual improvement was noted postoperatively. However, in five cases, visual acuity did not improve near normal (Beyond 0.5 logMAR) due to associated ocular comorbidities present before the surgery [Table 2]. In one case, visual acuity did not change (Pre: 2.3 logMAR vs. Post: 2.3 logMAR) post-surgery due to pre-surgery corneal decompensation. In two cases of amblyopia, visual acuity improved to 0.8 and 0.6 logMAR from 1.6 to 1.9 logMAR, respectively. In one eye where dislocated IOL was associated with resolved endophthalmitis, the visual acuity improvement of 1.0 logMAR from 1.9 logMAR was noted. In one eye with a history of macular hole surgery, vision improved to 0.6 logMAR from 1.9 logMAR. Nivean et al. have reported a single case with secondary aphakia who had undergone implantation of CM T flex IOL where his vision improved to 6/6 (P) from hand movement (HM).[13] In another study by Madanagopalan et al., they evaluated the outcomes of sutureless scleral-fixated lens to eliminate extraocular haptic manipulation where improvement in mean visual acuity from 0.34 logMAR (Range: 0.2–1.0) to 0.22 logMAR (Range: 0.0–0.77) was noted.[14] Increase in IOP has been documented post SFIOL implantation; however, in our study, the IOP was within normal range. In our series, we did not find any IOL-related post-operative complication. Furthermore, we did not encounter any case of retinal complications such as retinal detachment, cystoid macular edema, or vascular occlusions. This could be explained by the pars plana vitrectomy that was carried out during the surgery and endolaser done wherever required. However, one patient developed choroidal detachment postoperatively which can be attributed to hypotony caused by improper closure of scleral pockets or by direct damage to ciliary vessels from sharp instruments.[21,22] The patient was managed conservatively with oral and systemic steroids, which helped subside the choroidals over a period of one month. Two patients had dispersed hemorrhage, which self-resolved with topical medications.
| Age | Eye | Gender | cause | Pre BCVA logMAR | Pre surgery ocular co morbidity | Pre IOP | Post BCVA logMAR | Post IOP | Corneal edema | Haptic related complications | IOL stability | IOL centration | Endophthalmitis | Retinal Complication |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 12 | Right | Female | Subluxated Lens (Marfans) | 1.60 | Amblyopic | 12 | 0.80 | 14 | No | None | stable | well centered | no | no |
| 42 | Right | Male | Nucleus drop | 1.90 | Amblyopic | 17 | 0.60 | 19 | No | None | stable | well centered | no | no |
| 22 | Right | Female | Subluxated IOL | 2.30 | Corneal decompensation | 20 | 2.30 | 22 | Present | None | stable | well centered | no | no |
| 74 | Left | Male | Dislocated IOL | 1.90 | S/P PPV endophthalmitis | 20 | 1.00 | 22 | No | None | stable | well centered | no | no |
| 73 | Right | Female | IOL drop | 1.90 | Macular Hole | 16 | 0.60 | 14 | No | None | stable | well centered | no | no |
IOP: Intra ocular pressure, IOL: Intraocular lens, logMAR: log (Minimum angle of resolution), PPV: Pars plana vitrectomy, BCVA: Best corrected visual acuity
In our experience, we had difficulty grasping of T-shaped haptic in the initial two cases; however, later, we did not encounter any such problem. Various factors contribute to the learning curve, such as surgeon experience and specialty, that is, anterior versus posterior segment.[6,23,24] SFIOLs have been successfully implanted by both anterior segment and posterior segment surgeons; however, the latter might have an advantage in these scenarios due to their ability in managing intra- and post-operative complications.[6] In our series, all surgeries were performed by an experienced vitreoretinal surgeon. It can be attempted by anterior segment surgeon; however, care needs to be taken while haptics are being guided out with the help of forceps. As this is not a routine procedure, there is a chance that an inexperienced anterior segment surgeon may lose the grasp of the haptic and cause IOL dislocation. Furthermore, the surgery type is crucial in the assessment of the learning curve. With the sutured SFIOL implantation technique, there is always a risk of suture breakage. With sutureless techniques, there is difficulty in threading the trailing haptic into the needle, risk of haptic breakage, difficulty externalizing the haptic from scleral pockets, and risk of haptic burn during cautery. The novel CM T flex IOL is a single-piece IOL with a “T”-shaped haptic which allows easy grasping and externalization of haptics from sclerotomy. Furthermore, the haptic design eliminates the need for any suturing or tucking thus making it less traumatic.
Handling of the IOL during implantation is really crucial and care needs to be taken while loading the IOL in the injector and during the externalization of the “T” haptics. A previous study by Rouhette et al.[25] of similar IOL has reported IOL damage in 12.5% of the cases. However, in the present case series, we did not had any intraoperative haptic breakage or damage.
In our experience, we suggest that the corneal entry with keratome should not be superior (12 o’clock) but can rather be made at an obtuse angle (superotemporal for the right eye and superonasal for the left eye, i.e., 10 o’clock) for easier grasping of T junction of IOL with the forceps. Insertion of the MVR blade plays an important role in stabilizing the T junction. Insertion of the MVR blade must be made perpendicular to the limbus so that the “T” junction of the IOL snugly fits in the sclerotomy sites. Furthermore, it is important to hold the lens at the T junction to avoid intraoperative breakage of haptic. “T”-shaped haptic is externalized through the 23G sclerotomy site and left under the scleral bed without any tucking or suturing, thus reducing the chances of haptic exposure, knot-related complications, and IOL dislocation.
As this is a retrospective study design, endothelial cell density data was not available for analysis. Furthermore, post-surgery tilt of the IOL could not be measured; however, IOL stability and centration were documented clinically using a slit lamp. The study reports the short-term outcomes of single-piece SFIOL. The sample included in this series was heterogenous; however, in future studies, a homogenous group with a larger sample size and long-term follow-up could be considered as this would provide more insight toward long-term complications, if any.
CONCLUSION
Thus, we conclude that SFIOL with “T”-shaped haptic is a viable option for aphakic cases with inadequate capsular support. IOL implantation with “T”-shaped haptic is sutureless, less damaging to ocular structures, and has a shorter learning curve, making it easier for surgeons.
Ethical approval
The research/study approved by the Institutional Review Board at Institutional Ethics Committee, Isha Netralaya, number 2023/01, dated June 23.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Videos available on:
Financial support and sponsorship
Nil.
References
- Sutureless intrascleral posterior chamber intraocular lens fixation. J Cataract Refract Surg. 2007;33:1851-4.
- [CrossRef] [PubMed] [Google Scholar]
- Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124:1136-42.
- [CrossRef] [PubMed] [Google Scholar]
- Glued intrascleral haptic fixation of an intraocular lens. Indian J Ophthalmol. 2017;65:1370-80.
- [CrossRef] [Google Scholar]
- Extraocular needle-guided haptic insertion technique of scleral fixation intraocular lens surgeries (X-NIT) Indian J Ophthalmol. 2017;65:747-50.
- [CrossRef] [PubMed] [Google Scholar]
- Trans-scleral plugs fixated FIL SSF IOL: A review of the literature and comparison with other secondary IOL implants. J Clin Med. 2023;12:1994.
- [CrossRef] [PubMed] [Google Scholar]
- Scleral-fixated intraocular lenses: Past and present. J Vitreoretin Dis. 2017;1:144-52.
- [CrossRef] [PubMed] [Google Scholar]
- Comparative evaluation of suture-assisted and fibrin glue-assisted scleral fixated intraocular lens implantation. J Refract Surg. 2012;28:249-52.
- [CrossRef] [PubMed] [Google Scholar]
- Long-term outcome of combined pars plana vitrectomy and scleral fixated sutured posterior chamber intraocular lens implantation. Am J Ophthalmol. 2006;141:308-12.
- [CrossRef] [PubMed] [Google Scholar]
- Simplified and safe method of sutureless intrascleral posterior chamber intraocular lens fixation: Y-fixation technique. J Cataract Refract Surg. 2014;40:2-7.
- [CrossRef] [PubMed] [Google Scholar]
- Complications and visual outcomes after glued foldable intraocular lens implantation in eyes with inadequate capsules. J Cataract Refract Surg. 2013;39:1211-8.
- [CrossRef] [PubMed] [Google Scholar]
- Novel yamane technique modification for haptic exposure after glued intrascleral haptic fixation. Am J Ophthalmol Case Rep. 2019;14:101-4.
- [CrossRef] [PubMed] [Google Scholar]
- Exposure of haptic of posterior chamber intraocular lens after sutureless intrascleral fixation. BMC Ophthalmol. 2015;15:102-4.
- [CrossRef] [PubMed] [Google Scholar]
- CM T-Flex intraocular lens an innovative design for aphakia secondary to postcataract surgery. TNOA J Ophthalmic Sci Res. 2020;58:30.
- [CrossRef] [Google Scholar]
- A novel sutureless scleral-fixated lens that eliminates extra ocular haptic manipulation: The CM-T flex lens. Ophthalmic Surg Lasers Imaging Retina. 2020;51:648-50.
- [CrossRef] [PubMed] [Google Scholar]
- Primary or secondary anterior chamber lens implantation after extracapsular cataract surgery and vitreous loss. Eye. 1991;5:694-8.
- [CrossRef] [PubMed] [Google Scholar]
- Anterior chamber lens implantation after vitreous loss. Br J Ophthalmol. 1989;73:596-9.
- [CrossRef] [PubMed] [Google Scholar]
- Iris-claw intraocular lens implantation in various clinical indications: A 4-year study. J Clin Med. 2021;10:1199.
- [CrossRef] [PubMed] [Google Scholar]
- Five-year follow-up of secondary iris-claw intraocular lens implantation for the treatment of aphakia: Anterior chamber versus retropupillary implantation. PLoS One. 2019;14:e0214140.
- [CrossRef] [PubMed] [Google Scholar]
- Retropupillary fixation of iris-claw lens in visual rehabilitation of aphakic eyes. Indian J Ophthalmol. 2016;64:743-6.
- [CrossRef] [PubMed] [Google Scholar]
- Visual outcome and complications of various techniques of secondary intraocular lens. Oman J Ophthalmol. 2017;10:198-204.
- [CrossRef] [PubMed] [Google Scholar]
- Suprachoroidal hemorrhage following sutureless scleral-fixated intraocular lens-A case series. Saudi J Ophthalmol. 2023;37:60-2.
- [CrossRef] [PubMed] [Google Scholar]
- Retropupillary fixation of iris-claw intraocular lens versus trans-scleral suturing fixation for aphakic eyes without capsular support. J Egypt Ophthalmol Soc. 2015;108:157.
- [CrossRef] [Google Scholar]
- Surgical outcomes, complications and learning curve of glued intraocular lens of a vitreo retinal fellow in training. Indian J Ophthalmol. 2020;68:78-82.
- [CrossRef] [PubMed] [Google Scholar]
- A comparative study of transscleral suture-fixated and scleral-fixated intraocular lens implantation. Int Ophthalmol. 2019;39:839-45.
- [CrossRef] [PubMed] [Google Scholar]
- FIL-SSF Carlevale intraocular lens for sutureless scleral fixation: 7 recommendations from a serie of 72 cases. MICA study (multicentric study of the carlevale IOL) J Fr Ophtalmol. 2021;44:1038-46.
- [CrossRef] [PubMed] [Google Scholar]




