
Translate this page into:
Dexamethasone implant for the treatment of cystoid macular edema secondary to gyrate atrophy in an elderly patient

*Corresponding author: Jaydeep Avinash Walinjkar, Department of Vitreo-Retina, Shree Ramkrishna Netralaya, Thane, Maharashtra, India. drjaydeep23@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Walinjkar JA, Patel AQ, Natarajan S. Dexamethasone implant for the treatment of cystoid macular edema secondary to gyrate atrophy in an elderly patient. J Ophthalmic Res Pract. doi: 10.25259/JORP_28_2024
We report a 76-year-old woman presenting to our retina department for an ophthalmic evaluation. Her best corrected visual acuity (BCVA) was 6/18, N8 in both eyes (BEs). Her medical history revealed hypertension, cardiac disorder, and dyslipidemia for more than 15 years. Plasma amino acid testing showed an elevation in the amino acids, including ornithine. BE had been operated for cataract 10 years back. BE fundus [Figure 1a and b] showed multiple chorioretinal patches, bony spicules, and cystoid macular edema (CME). Optical coherence tomography [Figure 1c and d] of the macula showed cystoid spaces and a disrupted ellipsoid zone. Fundus fluorescein angiography showed a petaloid pattern in the late phase [Figure 2a and b]. All the other causes of CME in that age group were ruled out. A diagnosis of bilateral gyrate atrophy (GA) with CME was made. She was treated with an intravitreal dexamethasone implant (Ozurdex®, 700 μg) for BE (left eye [LE] followed by right eye). After 1 month, CME was resolved [Figure 2c and d], but the BCVA was maintained to 6/18, N6. On her last follow-up, i.e., after 1 year, visual acuity was stable, no recurrence of CME, and increase in intraocular pressure was noted.
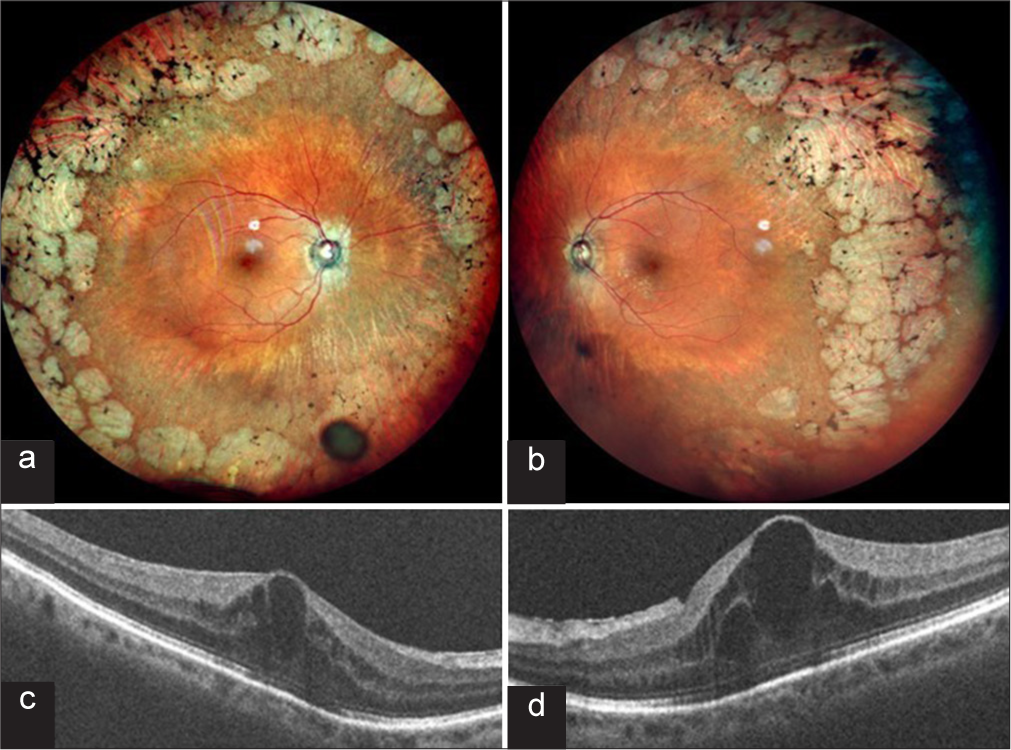
- A 76-year-old lady, a known case of gyrate atrophy presented to us showing (a and b) multiple, peripheral discrete patches of chorioretinal atrophy along with bony spicules. (c and d) Optical coherence tomography showing cystic spaces suggestive of cystoid macular edema.
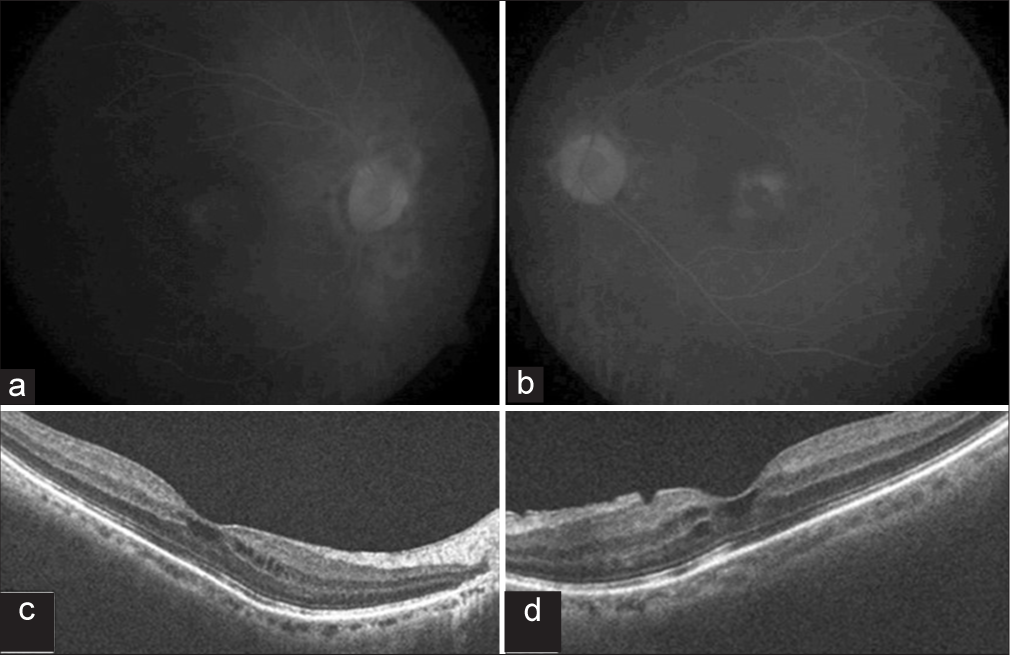
- (a and b) Fundus fluorescein angiography late phase demonstrating petaloid pattern suggestive of cystoid macular edema. (c and d) One month after dexamethasone implant showing significantly resolved cystoid macular edema.
GA is an autosomal recessive chorioretinal degeneration that is known to occur due to a mutation in the OAT gene.[1] Macular edema is the most common complication of GA.[2]
This may exacerbate the deterioration in vision. GA can be diagnosed clinically. However, genetic study does play a critical role in the diagnosis of inherited retinal dystrophies. The clinical features of GA include discrete patches of chorioretinal atrophy 360° in the periphery, which can eventually progress to the macula. In addition, bony spicules, epiretinal membrane (ERM), and foveoschisis can be seen.[3] The degree of macular edema and visual acuity may not always possess a correlation due to underlying degenerative retinal conditions.[3,4] Multiple factors can give rise to CME in elderly patients such as pseudophakia (typically occurs 4–6 weeks after cataract surgery), any occlusive (central retinal vein occlusion, ocular ischemic syndrome, diabetic retinopathy) or inflammatory event, age-related macular degeneration, vitreoretinal interface disease (ERM in LE was thin), and medications (prostaglandin analogs, mat epinephrine or related compounds, paclitaxel or other chemotherapeutics, nicotinic acid).[5] No such factors were present in our case. Many treatments have been suggested for GA-associated CME. Primary treatment includes dietary changes (arginine-restricted diet).[6] Secondarily, carbonic anhydrase inhibitors and corticosteroids such as intravitreal triamcinolone acetonide or dexamethasone implants can be utilized to treat CME.[6]
CME is commonly observed in young adults associated with GA. On the contrary, our patient showed macular involvement at a later stage in life. We did not find any other cause for the CME in her age group. We can conclude that CME secondary to GA may occur irrespective of age.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- The ornithine aminotransferase (OAT) locus: Analysis of RFLPs in gyrate atrophy. Am J Hum Genet. 1988;42:365-72.
- [Google Scholar]
- Cystoid macular edema secondary to gyrate atrophy in a child treated with sub-tenon injection of triamcinolone acetonide. Rom J Ophthalmol. 2018;62:246-9.
- [CrossRef] [PubMed] [Google Scholar]
- Ultrawide field fluorescein angiogram in a family with gyrate atrophy and foveoschisis. Oman J Ophthalmol. 2016;9:104-6.
- [CrossRef] [PubMed] [Google Scholar]
- Macular edema associated with gyrate atrophy managed with intravitreal triamcinolone: A case report. Arq Bras Oftalmol. 2007;70:858-61.
- [CrossRef] [PubMed] [Google Scholar]
- Macular profile of eyes developing macular holes in cases of central retinal vein occlusion treated with bevacizumab. J Kathmandu Med Coll. 2020;9:13-9.
- [CrossRef] [Google Scholar]
- Arginine-restricted therapy resistant bilateral macular edema associated with gyrate atrophy. Case Rep Ophthalmol Med. 2015;2015:137270.
- [CrossRef] [PubMed] [Google Scholar]




