
Translate this page into:
Peripheral giant cell granuloma of orbit: A case report

*Corresponding author: Lani Bhattacharyya, Department of Ophthalmology, Lakhimpur Medical College and Hospital, Lakhimpur, Assam, India. lanibhattacharyya@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Bhattacharyya L, Bhuyan J. Peripheral giant cell granuloma of orbit: A case report. J Ophthalmic Res Pract. 2024;2:32-4. doi: 10.25259/JORP_45_2023
Abstract
Giant cell reparative granuloma (GCRG) is a rare locally aggressive benign lesion of orbit with a total of less than 15 reported cases worldwide. A 35-year-old male presented with a left upper eyelid mass. Contrast-enhanced computed tomography orbit revealed a soft-tissue density lesion of the extraconal compartment of the left orbit. Wide local excision was done. Histopathology showed peripheral giant cell granuloma of the orbit with fibroosseous component. No recurrence has been seen after eight months. Definite diagnosis of GCRG is only possible by excision biopsy. Early intervention is important to differentiate from malignant lesion.
Keywords
Peripheral giant cell granuloma
Orbital tumor
Benign tumor

INTRODUCTION
Giant cell reparative granuloma (GCRG) is a locally aggressive benign reactive lesion. The occurrence of GCRG in the orbit is extremely uncommon and was first documented by Sood et al. in 1967.[1] Although trauma and chronic inflammation are thought to be contributing factors, the etiology is yet unknown. It is seen more among females in the first to third decades, in the epiphyses of the long bones (more than 97% cases), skull (about 2% cases): commonly maxilla and mandible. The other cranial bones seldom affected are petrous, sphenoid, ethmoid, and orbit.[2] Literature review has revealed 13 cases of GCRG having orbital involvement[3] and intracranial involvement in two of them.[4,5] Present case is reported by virtue of its rare occurrence, especially in India.
CASE REPORT
A 35-year-old male presented with gradual, progressive, painless left upper orbital mass since 1 month with no signs of proptosis, diminution of vision, or double vision. He did not give a history of any previous inflammation, sinusitis, or injury. Examination revealed a well-circumscribed 2 × 1 cm smooth, firm, irreducible, and non-tender mass in the superomedial quadrant of the orbital margin [Figure 1]. No notable influence on eye movement, intraocular pressure (IOP), visual acuity, and fundus were seen. General physical examination and routine blood tests, including serum calcium or parathyroid hormone (PTH) levels, were within normal limits. Contrast-enhanced computed tomography (CECT) revealed a well-defined 22 × 11 mm homogeneously enhancing soft-tissue lesion in the superomedial aspect of the extraconal compartment of the left orbit without bone erosion [Figure 2].
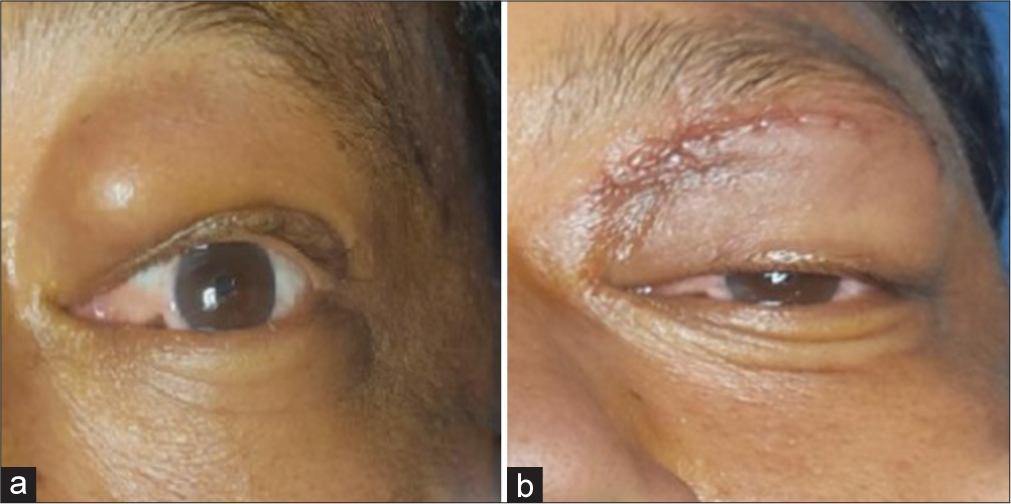
- (a) Left upper orbital mass and (b) immediate postoperative.
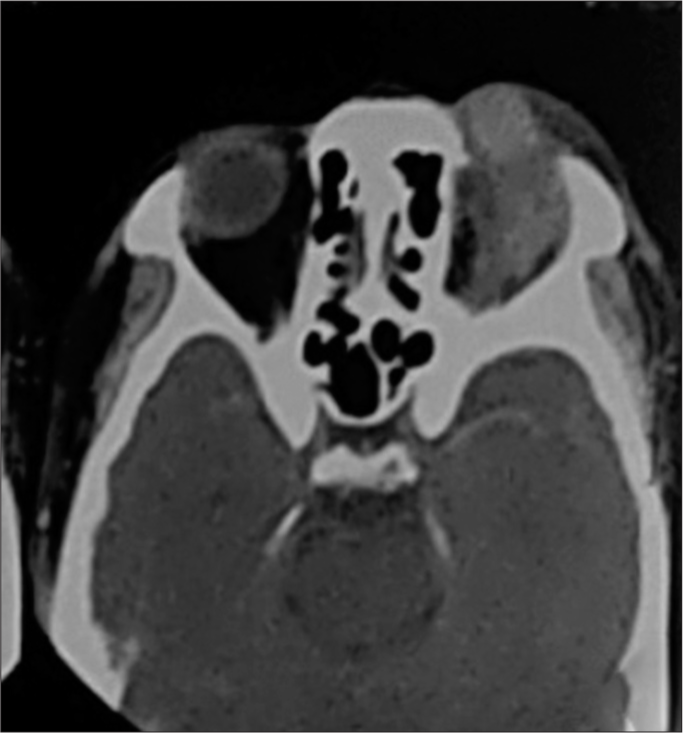
- Contrast enhanced computed tomography shows homogeneously enhancing soft tissue lesion in the left orbit without bone erosion.
Wide local excision of the mass en bloc along with the capsule was done from the subperiosteal space with curettage of 1 mm additional margin. Histopathology revealed a well-circumscribed encapsulated lesion comprising of fibrous tissue proliferation with fragments of osteoid and some osteoclastic giant cells. Stroma shows chronic inflammatory infiltration of lymphocytes with lymphoid follicle formation [Figure 3a and b]. Post-excision CECT showed no remnants. The patient is doing well, and no recurrence has been seen after 1 year of treatment clinically.
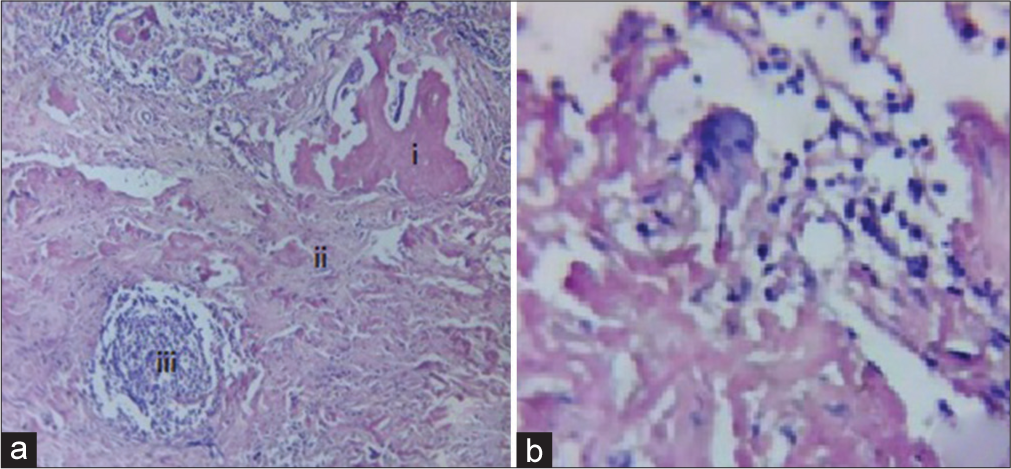
- (a) Well-circumscribed encapsulated lesion comprising of (i) osteoid fragments, (ii) fibrous tissue and lymphocytes in the stroma with osteoclastic giant cells, and (iii) lymphoid follicle; (b) osteoclastic giant cell.
DISCUSSION
Jaffe first elaborated GCRG in 1953, in the mandible and maxilla, prior to which they were classified under giant cell tumor.[6] They may occur in all age groups, more commonly in young adults and children, with female preponderance (2:1).[2] GCRGs are of two subtypes - central and peripheral. The central type of GCRG is bone-based and seen in the maxilla, mandible, and long bones. The peripheral subtype is soft-tissue-based, occurring in the oral cavity and sinus mucosa. Imaging reveals osteolytic lesions having an expansive nature, though quite varied and non-specific. Histopathology reveals a collection of large multinucleated osteoclast-like giant cells which tend to assemble around hemorrhagic foci.[7,8]
The definitive treatment of these lesions is excision biopsy. Adjuvant therapy in unresectable or remnant cases includes radiotherapy, calcitonin, corticosteroids, imatinib, bisphosphonates, and interferon-α. Radiotherapy is mostly avoided due to reports of malignant transformation post-radiation.[2,9] De Lange reported limited regression of lesions with interferon-alpha and imatinib without complete resolution.[10] Denosumab (monoclonal antibody against RANKL) is an alternative adjuvant therapy giving promising results in inoperable or locally advanced cases.[11] However, denosumab treatment duration and long-term effects require further evaluation.[12] In our case, the mass was removed in toto without any remnant, adjuvant therapy was not administered.
GCRG has to be distinguished from malignant lesions like osteoclastoma, aneurysmal bone cyst, ‘brown tumors’ found in hyperparathyroidism, Langerhans cell histiocytosis, and non-ossified fibroma. The recurrence rate of GCRG after complete resection is less than 10%. GCRG is differentiated from brown tumors by serum calcium, phosphorus, and PTH levels. Osteoclastoma is a giant cell tumor inside the bone, typically in the epiphysis of long bone having uniformly scattered giant cells having up to 50 nuclei and conspicuous mitotic figures with less apparent fibroblasts and osteoid while, in GCRG, the multinucleated cells are smaller, irregular with osteoid formation. Langerhans cell histiocytosis and aneurysmal bone cysts are excluded by the absence of Langerhans cells and cystic blood-filled vascular channels.[9]
CONCLUSION
GCRG of the orbit may present a diagnostic dilemma to oculoplastic surgeons due to overlapping clinical and radiological features with similar bony lesions. Histopathologic evaluation is obligatory to clinch the diagnosis. Thorough curettage and excision are the most potent therapies for GCRG and are effective in reducing recurrence.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Reparative granuloma of the orbit causing unilateral proptosis. Am J Ophthalmol. 1967;63:524-7.
- [CrossRef] [PubMed] [Google Scholar]
- Giant cell reparative granuloma of the orbit. Ophthalmic Plast Reconstr Surg. 2013;29:e94-5.
- [CrossRef] [PubMed] [Google Scholar]
- Giant cell reparative granuloma of the orbit. Ophthalmic Plast Reconstr Surg. 2005;21:463-5.
- [CrossRef] [PubMed] [Google Scholar]
- Giant cell granuloma of the orbit with intracranial extension. Neurosurgery. 1985;16:75-8.
- [CrossRef] [PubMed] [Google Scholar]
- Giant cell (reparative) granuloma of the orbit. Ophthalmology. 1981;88:1361-6.
- [CrossRef] [PubMed] [Google Scholar]
- Giant-cell reparative granuloma, traumatic bone cyst, and fibrous (fibro-oseous) dysplasia of the jawbones. Oral Surg Oral Med Oral Pathol. 1953;6:159-75.
- [CrossRef] [PubMed] [Google Scholar]
- Giant cell reparative granuloma of the orbit: Clinicopathological characteristics and treatment. Case Rep Ophthalmol Med. 2021;2021:4917968.
- [CrossRef] [PubMed] [Google Scholar]
- Locally aggressive orbital giant cell reparative granuloma in an infant: Case report and literature review. Int J Clin Exp Pathol. 2021;14:776-81.
- [Google Scholar]
- Multifocal central giant cell lesions of the maxillofacial skeleton: A case report. J Oral Maxillofac Surg. 1990;48:300-5.
- [CrossRef] [PubMed] [Google Scholar]
- Regression of central giant cell granuloma by a combination of imatinib and interferon: A case report. Br J Oral Maxillofac Surg. 2009;47:59-61.
- [CrossRef] [PubMed] [Google Scholar]
- Left orbital roof giant cell tumor of bone: A case report. Surg Neurol Int. 2018;9:127.
- [CrossRef] [PubMed] [Google Scholar]
- Current status and unanswered questions on the use of Denosumab in giant cell tumor of bone. Clin Sarcoma Res. 2016;6:15.
- [CrossRef] [PubMed] [Google Scholar]




