
Translate this page into:
Visual field defects in neurocysticercosis: A rare presentation

*Corresponding author: Amit S. Nene, Department of Vitreo-Retina, Isha Netralaya, Kalyan, Maharashtra, India. amitnene9@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nene AS, Rewatkar K, Bhat S, Shenoy P, Badole P, Shah S, et al. Visual field defects in neurocysticercosis: A rare presentation. J Ophthalmic Res Pract. 2024;2:70-2. doi: 10.25259/JORP_15_2024
Abstract
Neurocysticercosis is one of the commonest helminthic infections which affects central nervous system in humans and is caused by a tapeworm , Taenia solium. A 46-year-old male patient reported with complaint of restricted visual field in the left eye for one week. His best-corrected visual acuity was 6/6 partial, N6 in both eyes. Perimetry confirmed left homonymous hemianopia. The patient was referred to a neurophysician and based on magnetic resonance imaging brain and positron emission tomography scan, the patient was diagnosed with neurocysticercosis. The subject was started on oral medications following which the lesion resolved and improvement in visual fields was seen at one month follow-up. Ophthalmic manifestations of neurocysticercosis are variable and may include rare symptoms like visual field defects. A multimodal imaging and multidisciplinary approach can be helpful in the early diagnosis and faster recovery in patients with neurocysticercosis.
Keywords
Neurocysticercosis
Visual field defect
Seizure
Medical management
Taenia solium

INTRODUCTION
Neurocysticercosis is one of the commonest helminthic infections which affects central nervous system in humans and is caused by a tapeworm, Taenia solium. It is endemic in developing countries where poverty, unhealthy living conditions, and illiteracy are predominant.[1] Ocular manifestations of neurocysticercosis include proptosis, extraocular movement restrictions, internuclear ophthalmoplegia, orbital cellulitis, strabismus, ptosis, intraocular cyst, optic disc edema, retinal detachment, and vitreous hemorrhages.[2-6] Here, we report a rare case of neurocysticercosis presenting with visual field defects and its management.
CASE REPORT
A 46-year-old male patient reported with complaint of restricted visual field in the left eye for one week. His best-corrected visual acuity was 6/6p, N6 in both eyes, and color vision was normal. Intraocular pressure was 16 mm Hg in both eyes. Extraocular movements were full, free, and painless in all positions of gaze. The anterior segment revealed posterior polar cataract in both eyes. Pupils were round, regular, and reacting to light. Fundus examination showed attached retina with lasered lattice degeneration in both eyes. Optical coherence tomography of the macula was normal in both eyes [Figure 1]. On confrontation test, restriction in the outer limits of the visual field in the left side was noted. Perimetry confirmed left homonymous hemianopia [Figure 2].
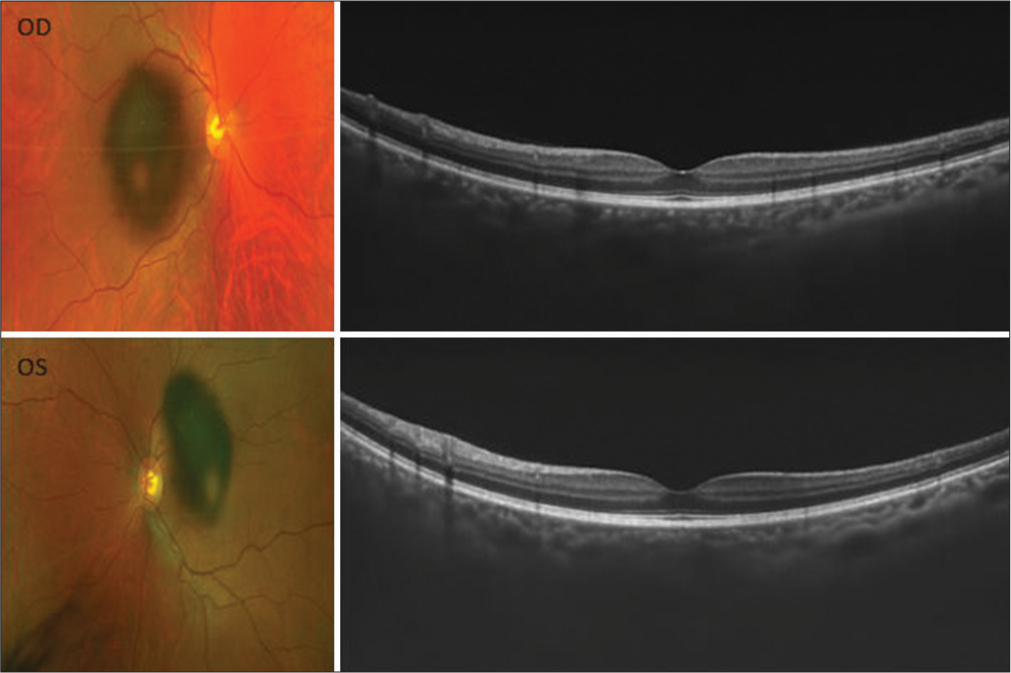
- Fundus photo (Left) and optical coherence tomography (Right) of right (Top) and left (Bottom) eye.

- Perimetry report showing left homonymous hemianopia in both eyes.
The patient was advised magnetic resonance imaging (MRI) brain + orbit where MRI brain revealed a few peripheral enhancing nodular lesions in the right occipital lobe (11 mm), largest measuring 13 × 12 × 7 mm and appearing as hypointense in T1 and isointense on fluid-attenuated inversion recovery with moderate perilesional edema [Figure 3a]. MRI orbit revealed prominence of peri-optic cerebrospinal fluid sleeves on both sides with partially empty sella. The patient was referred to neurophysician for further management where fluorodeoxyglucose positron emission tomography scan was done which revealed low-grade ring enhancing lesion (8 mm) with mild perilesional edema [Figure 3b]. A diagnosis of neurocysticercosis was made. Stool examination was normal with no larva seen. The patient was started on tablet Prednisolone 50 mg for 5 days and was gradually tapered over one month, tablet Albendazole 400 mg thrice a day for 21 days, and tablet Brivaracetam 50 mg twice a day for 60 days.

- (a) Magnetic resonance imaging brain and (b) fluorodeoxyglucose positron emission tomography scan illustrating neurocysticercosis. The black arrow shows cystic lesion.
At one month, MRI brain was repeated which showed resolving nodular lesion (3 mm) and reduced edema. Perimetry revealed significant improvement in the visual field defect [Figure 4]. The patient was continued on tablet Brivaracetam 50 mg twice a day by the neurophysician.

- Perimetry report showing improvement in visual field defect in both eyes.
DISCUSSION
Neurocysticercosis is a rare condition with an incidence ranging from 0.1% to 6% in Asian countries.[7] It is caused by a tapeworm , T. solium. Cysticercus, the larval form houses in humans and pigs who are the intermediate hosts whereas humans are definitive host for the adult tapeworm. When humans ingest uncooked infected pork, cysticerci get released by digestive enzymes and their scolices evaginate the intestinal wall where they multiply to form adult tapeworm.[1]
Seizure is the most common initial presentation seen in patients with neurocysticercosis.[8] In chronic cases, focal neurological signs can also be seen which are similar to brain tumor or tuberculomas with focal granulomatous etiology.[9] Acute stroke syndrome is also noted in few cases of neurocysticercosis.[10] The most common ocular symptoms include diplopia, decreased vision, redness, pain, and photophobia.[11] Lesion involving the optic nerve pathway in parietal, temporal, or occipital lobe can cause visual field defects or diminution of vision.[12]
The treatment modalities for neurocysticercosis include antiepileptics, corticosteroid, anthelmintic, and surgical interventions.[13] To the best of our knowledge, there is limited literature reporting visual field defects in cases of neurocysticercosis.[14-16] In our case, visual field defect was the initial presenting symptom. We noted improvement in the visual field defect following medical management which is in agreement with previous report by Besada et al.[15] Another study by Vaitheeswaran et al. has also reported improvement in visual fields post-orbitotomy which was carried out to remove optic nerve cysticercosis.[16]
CONCLUSION
Ophthalmic manifestations of neurocysticercosis are variable and may include rare symptoms like visual field defects. A multimodal imaging and multidisciplinary approach can be helpful in early diagnosis and faster recovery in patients with neurocysticercosis.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Neurocysticercosis presenting as isolated wall-eyed monocular internuclear ophthalmoplegia with contraversive ocular tilt reaction. J Neurosci Rural Pract. 2012;3:84-6.
- [CrossRef] [PubMed] [Google Scholar]
- Ocular cysticercosis with vitreous hemorrhage: A rare complication of a common disease. Springerplus. 2015;4:217.
- [CrossRef] [PubMed] [Google Scholar]
- Worm in the eye: A case report of ocular neurocysticercosis with adherent retinal cyst. Cureus. 2023;15:e50194.
- [CrossRef] [Google Scholar]
- Disseminated neurocysticercosis with bilateral papilledema: A case report. J Med Case Rep. 2019;13:2-5.
- [CrossRef] [PubMed] [Google Scholar]
- Multiple brain parenchymal neurocysticercosis with extraocular muscle cysticercosis affecting levator palpebral superioris and superior rectus complex: An unusual association. BMJ Case Rep. 2013;2013:bcr2012007421.
- [CrossRef] [PubMed] [Google Scholar]
- Taenia solium taeniosis/cysticercosis in Asia: Epidemiology, impact and issues. Acta Trop. 2003;87:53-60.
- [CrossRef] [PubMed] [Google Scholar]
- A systematic review of the frequency of neurocyticercosis with a focus on people with epilepsy. PLoS Negl Trop Dis. 2010;4:e870.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical manifestations associated with neurocysticercosis: A systematic review. PLoS Negl Trop Dis. 2011;5:e1152.
- [CrossRef] [PubMed] [Google Scholar]
- Cerebrovascular complications of neurocysticercosis. Neurologist. 2012;18:17-22.
- [CrossRef] [PubMed] [Google Scholar]
- Ocular and orbital cysticercosis. Acta Ophthalmol Scand. 2001;79:408-13.
- [CrossRef] [PubMed] [Google Scholar]
- Homonymous hemianopia: Challenges and solutions. Clin Ophthalmol. 2014;8:1919-27.
- [CrossRef] [PubMed] [Google Scholar]
- Neurocysticercosis: A review of current status and management. J Clin Neurosci. 2009;16:867-76.
- [CrossRef] [PubMed] [Google Scholar]
- Disseminated neurocysticercosis presenting as isolated acute monocular painless vision loss. J Neurosci Rural Pract. 2014;5(Suppl 1):S89-92.
- [Google Scholar]
- Bilateral disk edema with unilateral macular serous fluid secondary to neurocysticercosis. Optometry. 2005;76:239-49.
- [CrossRef] [PubMed] [Google Scholar]
- Minimally invasive bone-saving orbitotomy for removal of optic nerve cysticercosis. Orbit (London). 2015;34:109-11.
- [CrossRef] [PubMed] [Google Scholar]




